|
1) Always ensure that you have salad with your meal, whether your meal consists of bread, rice or pasta.
It is important to have your 5 A DAY (fruits and vegetables) as they are a great source of Vitamins especially Vitamin C. It is also a good mineral source and are low in fat and calories. They are also a good source of fibre which helps maintain the digestive system and prevent constipation and lowers the probability risk of heart problems, diabetes, stroke and certain cancers such as bowel cancer. Tomatoes, cucumbers, leeks, red peppers, green peppers, sweetcorn and the list can continue! 2) Make smoothies! This is another method in how to get your 5 A DAY. Instead of fizzy drinks and squash. Why don’t you combine your favourite fruits or vegetables together and make a smoothie? HOWEVER, try to ensure that you drink 1 glass (150ml) only as when the fruits or vegetables are blended, it releases the natural sugars contained within the fruits and can damage the teeth! 3) Breads, rice and pasta contain starch! Eating wholemeal bread, pasta and brown rice is a suitable option to improve the digestive system as it has a high content of fibre.There is different types of fibre: soluble and insoluble that has an impact on one’s body in varied manners. Wholemeal bread etc is an example of insoluble fibre. Insoluble fibre cannot be digested and passes through the intestines without being broken down. Its role is to aid other foods pass through the digestive system with ease preventing digestive problems. Studies have shown that those that eat wholegrain breads, porridge and cereals daily, lowers the risk of bowel cancer by 20%. However, if you have diarrhoea, please try to lower the amount of insoluble fibre diet. Soluble fibre on the other hand lowers cholesterolin levels in the blood. It can be digested by the body. Examples include fruits, vegetables, linseeds and oats, if you experience constipation; steadily increase the number of soluble fibre within your diet – this will aid in stools to pass through your gut. Nevertheless, if you have irritable bowel syndrome (IBS) or any other digestive orders – the amount and type of fibre within your meal need to modified and is dependent on the symptoms you experience. Thus, it is better for your own G.P to advise you further as he/she contains your clinical history and details.
1 Comment
Last week we looked at the benefits of black seed oil. This week we will look at the benefits of honey.
The earliest records of beekeeping were in Cairo in 2400BC. The Ancient Egyptians used it as a sweetener and embalming fluid whereas the Ancient Greeks observed honey as a healing medicine as well as important food as well as other countries in Europe. However when sugar arrived, the usage of honey as a sweetener was reduced; instead it was employed for wounds, gastrointestinal diseases, cardiovascular-related and liver-related issues. So what’s inside Honey? Honey primarily consists of two sugars: fructose (disaccharide) and glucose (monosaccharide). Other constituents include oligosaccharides, minerals, amino acids, vitamins and enzymes. In addition, honey contains chemicals that work effectively as an synergistic antioxidant such as flavonoides, catalase, ascorbic acid and others. Benefits of Honey A) Anti-microbial activity Bacteria Honey can exhibit anti-bacterial activity against bacteria such as Helicobacter pylori, Escherichia coli, Shigella and Salmonella. A study has shown that honey is effect as prenisolone treatment when used in colitis. A hospital-based bacterial infection called MRSA; there has been studies were honey has shown antimicrobial activity under in-vitro conditions. Another study examined the effects of honey on patients with UTI (urinary tract infections) that is normally caused by bacteria such as E.coli, S.faecalis and Proteus species. Results show that honey is effective as these type of bacteria are sensitive to honey due to its antibacterial activity. As you can see from the above examples that honey is effective against bacterial infections; the question is how? This is linked to its properties stated below: 1) Honey contains hydrogen peroxide which is synthesised by glucose oxidase that allows anti-bacterial activity to occur. 2) The amount of sugar in honey hinders bacterial growth (bactericidal) but is not the only reason for honey’s anti-bacterial activity as honey contains lysozymes, organic acids that also have anti-bacterial properties. 3) pH of honey is 3.2-4.5 – this is low acidity and is able to inhibit growth of majority of micro-organisms. Viruses Besides, anti-bacterial activity, honey also has anti-viral effects. Studies have shown that topical honey was effective compared to acyclovir cream in managing recurrent lesions caused by herpes virus. Another study reported that it has inhibitory effects on rubella virus. Fungus Honey is able to inhibit the growth of fungus as well production of toxins. Fungal infections such as cutaneous and superficial mycoses such as athletes foot and ringworm as well as for the treatment of dandruff and seborrheic dermatitis have been found to respond to honey. B) Anti-inflammatory activity. Studies have shown that honey has anti-inflammatory activity against wounds such as abscess, burns, amputation, surgical. Ulcers and perineum as well as other types of wounds. It stimulates healing mechanism by stimulating tissue regeneration, reducing inflammation and clearing infection. The molecular mechanism of healing the wounds is still being studied however the type of wound and degree of severity play important factors in its effectiveness. C) Honey and Heart diseases. In the developed world, the rates of disability, mortality and economic costs are high for Ischaemic Heart Disease (IHD) than other diseases. Myocardial infarction (MI) and Arrhythmias (ventricular arrhythmias such as tachycardia and fibrillation cause high mortality rates – thus anti-arrhythmic drugs are prescribed) are serious manifestations of IHD. Honey contains flavonoids which lowers the chance of cardiovascular diseases as it prevents low density lipoproteins (LDL) from oxidation, lower platelets’ ability in blood to clot and improve coronary vasodilation. It also has phenolic compounds that is really effective against coronary heart disease (CHD) due to its anti-oxidant, anti-ischaemic, vasorelaxant and anti-thrombotic properties. In addition, nitric oxide (NO) levels in honey have a protective effect against cardiovascular diseases. Moreover, honey is able to reduce the blood pressure in the veins which consequently lowers congestion. D) Honey and Cancer Some studies have shown that honey has anti-neoplastic activity in cancers such as bladder cancer. E) Gastrointestinal tract diseases Honey and Eye diseases Studies have shown that topical honey as ointment appears to be effective against opthalmological conditions such as keratitis, conjunctivitis, burns and corneal injuries. F) Honey and diabetes Honey is effective against Type I and II Diabetes as studies have shown it can lower plasma glucose levels, blood lipids, C-reactive protein and homocystein levels. It also appears honey stimulates insulin secretion and elevates haemoglobin concentration. Overall, there are many benefits of honey and before these studies have been performed; Allah has already revealed before mankind in the Glorious Quran: ‘Your Lord revealed to the bees: "Build dwellings in the mountains and the trees, and also in the structures which men erect. Then eat from every kind of fruit and travel the paths of your Lord, which have been made easy for you to follow." From inside them comes a drink of varying colours, containing healing for mankind. There is certainly a Sign in that for people who reflect.’ [16:69] Black Seed is a plant from Ranunculaceae (buttercup) family. It originates from Western Asia. It has white flowers when in bloom.
For over 2 centuries, black seed has been used by different cultures as a natural remedy for varied diseases and improve our health and well-being. Ancient Egyptians knew its benefits and called it a panacea (cure for illnesses) whereas the Ancient Romans utilized it as part of a diet and called it Greek Coriander. Ancient Greeks used it for aches of the head and teeth as well as nasal congestion. Our Beloved Prophet peace be upon him: ‘Use the Black Seed for indeed, it is a cure for all diseases except death.’ [Sahih Bukhari - 7:591] Current Research Studies have shown that its active ingredient, crystalline nigellone, contains 15 amino acids. Amongst these include 8 essential amino acids. It also has carbohydrates, fatty acids including linolenic and oleic acids, alkaloids, volatile oils, and dietary fibre, as well as minerals such as calcium, iron, sodium and potassium. Recent studies have shown that black seed is an antibiotic, anti-tumour, anti-inflammatory, anti-histaminic, anti-bacterial, anti-bronchial and immune-boosting agent. Some studies have shown it has trypanocidal properties and can stimulate the host immune system to maintain parasite proliferation. Consequently, it can help manage African sleeping sickness despite there is a risk of damage gradually occurring to host organs (shown due to increase in serum enzymes). What does Black Seed Oil contain? Black Seed Oil contains 3 main natural phytochemicals: thymoquinone (TQ), thymohydroquinone (THQ) and thymol. A study published in the Egyptian Journal of Biochemistry & Molecular Biology experimented these 3 natural chemicals against 30 human pathogens. Results suggested that all three chemicals showed 100% inhibition for these pathogens. Thymol - It is also present in thyme. It is a natural monoterpene. It is useful against fungus and viruses. Studies found it to be the best anti-fungal agent followed by TQ and THQ. It is also used in cosmetics and food flavouring. Thymoquinone - It has anti-tumour, anti-oxidant, anti-inflammatory properties. Studies have shown it to aid with asthma, diabetes, carcinogenesis and encephalomyelitis. It preserves anti-oxidant enzymes glutathione peroxidase and glutathione-S-transferase as they detoxify and aid in cellular anti-oxidant defense systems as they protect the liver from toxins. Thymohydroquinone - It is a natural acetylcholinesterase (AChE) inhibitors that aims to stop enzymatic activitity which increase the amount of neurotransmitter acetylecholine remains active in the brain. These AChE inhibitors treat Schizophrenia, Glaucoma, Alzheimer’s disease, apathy and other conditions. Top 10 Benefits of Black Seed Oil Benefit 1: Anti-Cancer activity. Thymoquinone and thymohydroquinone can aid in preventing cancer via the following methods: Anti-angiogenesis Anti-metastasis Cell cycle arrest Induces apoptosis Anti-proliferation Generate reactive oxygen species. Studies conducted on mice models revealed that thymoquinone combined with chemotherapy increase therapy and lower toxicity. Other studies have also been performed on the following types of cancer: Colon cancer – studies shown to inhibit growth of colon cancer cells with no side effects. Brain cancer – Studies have shown that thymoquinone can induce apoptosis in glioblastoma cells. Glioblastoma cells is one of the most aggressive brain tumours. Oral cancer – Studies have shown that thymoquinone can induce apoptosis in oral cancer cells. Leukaemia – Thymoquinone can induce apoptosis in leukaemia cells. Breast Cancer – Thymoquinone can induce tumour growth and apoptosis in breast cancer cells. Benefit Two: Hair Black Seed oil can restore hair loss and strengthens hair roots; studies are still being conducted as to reason behind it. However there are theories that it is due to anti-oxidant and anti-microbial properties. Benefit Three: Epilepsy Studies have found it to lower the amount of seizures in children who do not respond to conventional treatment. Benefit Four: Brain Damage Some studies have found that it can revese damage to the brain especially that caused by lead toxicity. Benefit Five: Protect against Heart Attack Studies have shown it protect the heart. Benefit Six: Infections Infections caused by bugs such as Methicillin resistant Staphylococcus aureus (MRSA) known to spread around hospitals. MRSA are staphylococcus bacterial infections that can resist to antibiotics. Elderly and Immunodeficient individuals are at risk. Studies have shown that black seed oil can remove these infections. Benefit Seven: Losing Weight Studies have shown that Black seed oil has anti-obesity and anti-inflammatory properties. It can reduce blood glucose, cholesterol and triglyceride levels. It can also lower appetite and glucose absorption in the intestines. Benefit Eight: Strengthens the liver. Studies have shown that it increases the function of liver and prevent both damage and disease. Individuals with poor liver function due to side effects of medications, consuming alcohol or disease; the role of black seed oil increases healing process. Benefit Nine: Diabetes Studies have shown that black seed oil aids in preventing type 1 and 2 Diabetes. A recent study revealed that black seed oil can cause gradual partial regeneration of pancreatic beta-cells (consequently increases beta-cell function in the pancreas), increases the lowered serum insulin concentrations and decreases the elevated serum glucose. Another study revealed that it can work efficiently as that of metformin drug to improve glucose tolerance. Alternatively, the difference is that there is no side effects with black seed oil, whereas metformin has a number of side effects: such as pain in the stomach and muscle and head, constipation, digestive problems etc. Benefit Ten: Skin There are many benefits of black seed oil on the skin and other cells. Studies have shown that Black Seed Oil has same effect on eczema as Betamethasone that is prescribed for eczema. There are so many other benefits of Black Seed Oil not so included. The involvement of Penicillium and Pseudomonas in the cause and/or cure of human microbial disease.4/29/2015 There are many microbes which humans have contact with everyday that are harmless; however, there are other microbes that cause disease known as pathogens. Penicillium is a genus of sac fungi called Ascomycota. Its cell wall is composed of chitin and its body known as thallus, has high-branched cell filaments of hyphae (Willey, 2008:p.631). These cellular characteristics give Penicillium strength to perform its applications. Pseudomonas is a gram-negative, rod-shaped proteobacteria. They have a lipopolysaccharide outermembrane whose role is to protect the bacteria from host defences by creating a permeable barrier (Willey, 2008:p.60). The Pseudomonas genus has 60 species and is divided into rRNA homology groups based on their properties such as pathogenicity because there are many species that can be positioned under one characterized group (Willey, 2008:p.556). Both microbes, Penicillium and Pseudomonas, are involved in the cause and/or cure of human microbial disease.
The involvement of Penicillium in microbial disease is the production of β-Lactam antibiotics called penicillin. Originally, P.notatum was used to make penicillin however; there are now other species like P.chrysogenum that manufacture penicillin in vast amount. These drugs are bactericidal because they tackle disease by binding to Penicillin-binding Proteins (PBPs) such as transpeptidase that are responsible for peptidoglycan crosslinkages. This enzyme-substrate complex inhibits the bacterial cell wall, losing its function but causes less damage to the host; this is known as selective toxicity (Willey, 2008:p.837). Phenoxymethylpenicillin (Penicillin V), is effective using this mechanism against gram-positive bacteria like Streptococcus pyogenes; a bacterium that causes skin infections. However, Phenoxymethylpenicillin is not very effective against gram-negative bacteria because they have a protective outermembrane and contain β-Lactamase enzyme that inactivates penicillin by hydrolysing a bond in β-Lactam ring. This emphasises the contribution of Penicillium to treatment of disease because its species are used to manufacture penicillin which are effective against diseases caused by gram-positive bacteria. Other penicillins are effective against gram-positive and gram-negative bacteria. For instance, Ampicillin is less susceptible to inactivation by gram-negative bacteria and inhibits transpeptidase competitively because this semi-synthetic drug is a modified version of the natural penicillin by an addition of an amino group. This emphasises the involvement of Penicillium in the cure of disease because the antimicrobial activity can vary with individual penicillins. Some are narrow-spectrum drugs that kill specific bacteria, others are broad-spectrum that effect different bacteria. The involvement of Pseudomonas in disease is causing them by three stages: attaching to bacteria, invading it and causing infections. The origins of Pseudomonas’ invasive infections are mainly due to its species; P.aeruginosa. P.aeruginosa is a nosocomial, antibiotic-resistant pathogen. People with Pseudomonas infections typically have low immune systems such as cystic fibrosis where Pseudomonas produces ‘slime’ in the lungs causing pneumonia (Singleton, 1995:p.286). Another infection caused by P.aeruginosa is ‘Hot Tub Rash’ the common name given to skin infection called dermatitis. It spreads via contaminated water which indicates how this pathogen can tolerate water environments and cause infection (CDC, 2010). This illustrates Pseudomonas’ contribution to disease because P.aeruginosa causes many pathogenic infections due to its cellular characteristics and ability to form biofilms which protects it from environmental factors. Other Pseudomonas species are involved in the treatment of human microbial disease. For instance, P. flourescens extracts are used to produce an antibiotic called Mupirocin. Mupirocin is effective against gram-positive bacteria like staphylococci to treat skin infections topically. For instance, impetigo that commonly affects children who have other skin problems because it is contagious (Lancini,1995:p.178). Studies on Mupirocin have shown that it inhibits isoleucy-tRNA synthetase enzyme which can affect protein synthesis in the bacterium (Capobianco, 1989). This indicates how Pseudomonas is able to produce antibiotics against other bacteria despite itself can cause bacterial diseases. Penicillin can cause adverse side effects such as allergies where the body produces antibodies that suspect penicillin as an antigen rather than a cure. The most severe allergic reaction is anaphylaxis where bronchi are narrowed causing breathing difficulties (Singleton, 1995:p.297). Other Penicillium spp. like P.marneffei causes disseminated infection called penicilliosis in normal immune individuals. These individuals commonly have their skin, lungs and gut infected where symptoms like lesions can be mistaken for histoplasmosis that occurs in AIDs patients. In other words, the symptoms of both infections ‘mimic’ each other (University of Adelaide, 2010). This emphasises the downside of Penicillium where penicillin causes side effects and cause disease. However, P.marneffei is the only dimorphic species in the Penicillium genus. Ultimately, microbes have major importance in disease, some can be pathogenic, and others can be beneficial to produce antimicrobial drugs. Both Penicillium and Pseudomonas are involved in the cause and cure of human microbial disease. However, Penicillium predominantly contributes to treatment of bacterial diseases but depends on its side chain that determines its effectiveness. Pseudomonas predominately causes infections due to its cellular characteristics that enable it to become antibiotic-resistant. In fact, Ticarcillin, semisynthetic penicillin is effective against P.aureginosa. Today, researchers aim to develop new semi-synthetic drugs to treat disease as the number of antibiotic-resistant microbes increase to help treat human microbial disease. References Capobianco,J., Doran,C., Goldman,R. (1989) ‘Antimicrobial Agents and Chemotheraphy: Mechanism of mupirocin transport into sensitive and resistant bacteria’ American Society For Microbiology: 33 (2): 156-163. Available online: http://aac.asm.org/cgi/content/abstract/33/2/156 Centre for Disease Control and Prevention (2010) ‘Hot Tub Rash’ Pseudomonas Dermatitis/ Folliculitis’ Available online: http://www.cdc.gov/healthyswimming/derm.htm Lancini, G., Parenti, F., Gualberto Gallo, G., (1995) ‘Antibiotics: A Multidisciplinary Approach’. New York: Plenum Press. pp.178 Singleton, P. (1999) ‘Bacteria in Biology, Biotechnology and Medicine’ 5th ed. England: John Wiley & Sons Ltd pp.286, 297 University of Adelaide (2010) ‘Mycology online: Penicilliosis marneffei’ Available online: http://www.mycology.adelaide.edu.au/Mycoses/Opportunistic/Penicilliosis_marneffei/ Willey,J., Sherwood, L., Woolverton,C. (2008) ‘Prescott, Harley, and Klein’s Microbiology’ 7th ed. New York: McGraw-Hill pp.60, 556,631,837. CF is caused by the abnormal functioning of the protein CF transmembrane conductance regulator (CFTR). CFTR is only expressed in a number of cells but all cells carry the gene for the protein. CFTR is mainly found in epithelial cells and in order for CFTR to be expressed a certain amount must be produced at the right time. The CFTR protein contains 1480 amino acids and is important in regulating the flow of chloride and sodium across the epithelial surface. The function of CFTR is disrupted by changes in the base sequence, these changes are called mutations. Over 1,200 mutations have been discovered for CF but the most common is deltaF508-which is a 3 base pair deletion (of amino acid phenylalanine) and account for 76% of affected chromosomes in the UK. CF is an autosomal recessive disease, so both CFTR genes are required for the individual to be diagnosed with CF, if only one is present then the individual will be a carrier. A classification system has been produced that characterises CFTR mutation depending on the effects the mutation has on the CFTR production. Class 1 are nonsense mutations as there is a premature stop codon which leads to the production of unstable mRNA or the release of incomplete proteins that are not functional. This protein is degraded before it can reach the membrane. The phenotype of patients carrying the stop mutation is severe. In Class 2 after CFTR has been translated into a peptide in the ribosome, it will go through a series of processes in the ER and Golgi apparatus. These processes are glycolisation and folding by chaperons that enable the trafficking of CFTR to the apical cell membrane. In Class 2 mutations, the CFTR protein is unable to fold correctly due to the deltaF508. The protein is retained in the ER and eventually targeted for degradation. Class 3- phosphorylation of CFTR protein by protein kinase (PK) & dephosphorylation by protein phosphatase (PP) is important in regulating CFTR chloride channel activity. Phosphorylation of the regulatory domain causes ATP to bind to the nucleotide binding domain (NBD) resulting in induction of chloride transport. In Class 3 CFTR is produced, processed and transported and inserted into the apical membrane however phosphorylation or binding of ATP does not occur. Class 4- in this class of mutation the CFTR protein is produced, processed, transported to the apical membrane. Phosphorylation and dephosphorylation also occur. In class 4, phosphorylation actually reduces chloride transport. Class 5- this class of mutations generates both abnormal and correctly spliced transcripts. These patients have a mild phenotype but with variable disease expression depending on the level of correctly spliced transcripts. Steps of diagnosing a baby with CF Neonatal screening test To diagnose a baby with CF the first test that is to be performed is the neonatal screening test. During the 1st 2 weeks of Childs life, high levels of IRT levels will be shown if CF is present. In this test a blood sample is taken from the child heel and the level of this pro-enzyme is monitored. If levels are high, then other genetic test can be carried out to find out exactly which mutations are present and detect the severity of the disease. This test is not reliable after 2 weeks of birth as several other factors may play a part in the high levels of IRT. PCR Analysis One of the 1st genetic tests that can be carried out for the diagnosis of CF is PCR analysis. This test is carried out to see if the most common mutation (deltaF508) is present which is the deletion of 3bp. PCR primers have been developed that can distinguish a normal gene from a mutant gene. With these primers a 154 bp product is produced from a normal individual and a 151 bp product is amplified from DNA of an individual with the disease. If this CF mutation is present it will show a distinct pattern from a normal pattern. If both genes have this mutation, two bands will be seen. If 1 band is present, this indicates that other the second gene has a different mutation which can be followed up by other genetic tests. Normal Carrier CF Individual Individual Individual ---------------------------------- 154 bp ___2x ___ 151 bp ___ ___2x ---------------------------------- ARMS Another test that can be performed is the amplification refractory mutation system (ARMS). This can be used to recognize the 20 most common CF mutations. In this technique, three multiplex PCR reactions are performed in parallel for each individual. Each tube contains number of separate primers capable of detecting different mutations. In each tube, sets of primer pairs are designed to anneal a particular allele to produce distinct band. A band is only produced in presence of mutant allele and the absence of the band indicates that the allele is absent; therefore positive signals are easily differentiated in order to identify the exact mutations present. Since it is possible for one of the tubes to produce no bands, there are always positive controls to show that the PCR reaction is functioning properly in each tube. The ARMS assay is accurate, rapid and easy to perform, but it does not distinguish between homozygotes and heterozygotes except for the DF508 mutation. Multiplex Allele Specific PCR Allele specific oligonucleotide (ASO) dot-blot is a widely used technique to diagnose CF. Genomic DNA from the patient is amplified by PCR and transferred onto nylon membranes as a dot-blot. Membranes are hybridized with either a radiolabelled wild type allele specific oligonucleotide (ASO) or mutated ASO. Following autoradiographic exposure, the combination of oligonucleotide hybridization is observed. Using this combination an ASO dot-blot can clearly distinguish homozygous, heterozygous and wild type subjects. 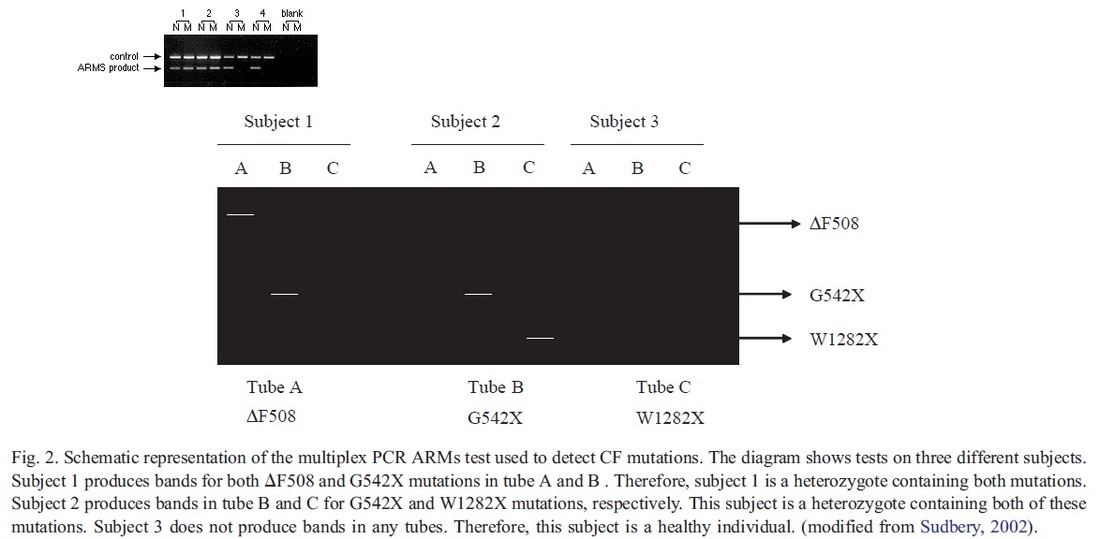 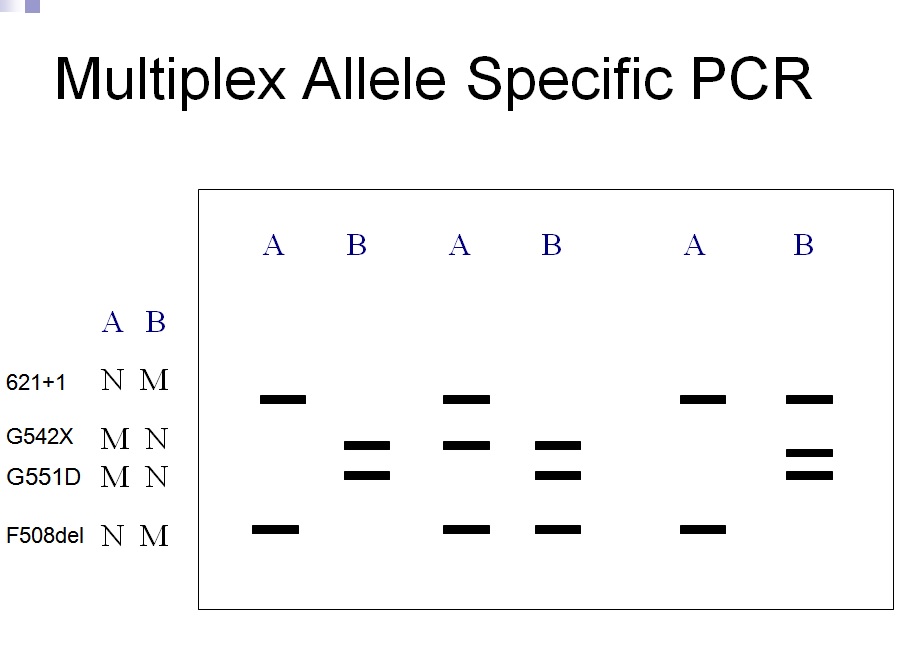
The molecular basis of DMD was first determined in the 1980s. DMD symptoms usually begin to show between the ages of 3-5 and affect 1 in 3,500 patients. At the age of 20 patients are usually unable to walk so bound to a wheelchair. In 1986 Gowers observed that familial cases were more common than sporadic cases. P.E Becker discovered that there is a milder form of DMD where symptoms usually show after the age of 12 and affects 3 per 100,000 new born. He also discovered that X-linked disorders have slower progression. It does not affect reading frame but has DMD gene deletions. The protein involved in DMD is dystrophin. The dystrophin gene is the largest gene that encompasses 206 million base pairs and contains 79 exons. It is the main proteins that link the cytoskeleton to the extracellular matrix. DMD has shown variation in muscle size and penetration of connective tissue. Patients suffering from DMD have a deletion of 45 exons and in BMD 35 exons. Deletions have been found on Xp21.
The cloning of the dystrophin gene in the 1980s led to the discovery of physiological consequences of DMD. There are three major proteins that were first discovered known as dystrophin associated protein complex (DAPC). Dystrophin is a rod shaped cytoplasmic proteins that links actin fibres in cortex of muscle cells to extracellular basal lamina (connective tissue) by forming a bridge between actin and transmembrane protein complex called (dystrophin-associated sarcoglycan complex) (DASC) located in sarcosplasma. Without dystrophin an improper complex is formed. DMD gene has 79 exons with promoter regions scatters across 2.4 Mb. The first of the proteins is known as dystroglycan. The dystroglycan complex is a membrane-spanning complex composed of two subunits, alpha- and beta-dystroglycan. Alpha-dystroglycan is a cell surface peripheral membrane protein which binds to the extracellular matrix (ECM), whereas beta-dystroglycan is an integral membrane protein which anchors alpha-dystroglycan to the cell membrane. The dystroglycan complex provides a tight link between the ECM and cell membrane. No patients have shown the mutation is the studies of Dalkillic et al (2003). The second proteins are Dystrobrevins and Syntrophins. These have been found to bind to dystrophin; these include multiple iso-forms of alpha and beta dystrobrevin and three syntrophin iso-forms. Alpha dystrobrevin is expressed in the skeletal muscle, and localized in the sarcelloma, and interacts with dystrophin. No mutations have been found but mice models with this mutation shown mild dystrophy. Three iso-forms of syntrophin have been expressed in the skeletal muscle and shown to interact with dystrophin and dystrobrevin, and bring (nNOS) nitric neurol oxide synthesis. nNOS cause vasodilation near the muscle tissue in order for blood flow to occur for contraction. Less syntrophin would mean less nNOS. No patients have shown to have this except studies of mice. Finally the last protein is the sarcoglycan-sarcospan complex. These forms of sarcoglycan interact with each other strongly that give rise to MD. DMD patients have shown to decrease in this protein and lost at the membrane. Other types of proteins that are involved are caveolac, and there is an abnormal size and number. This is found in all muscle types and interacts with C-terminal. DMD is an X-linked recessive disorder as the mutated gene is found on the X chromosome. The X chromosome is important for the development & growth. Females can be carriers of this disease if one X chromosome is affected as the other X chromosome would compensate. As for males they can either be normal with without the affected gene or affected. A female carrier can pass her affected X chromosome to son/daughter, therefore the son has a 50% of being infected and the daughter has 50% of being a carrier. There are strategies used to identify and isolate genes involved in this monogenic disorder. 1) Cytogenetic rearrangement results in DMD having location sub-chromosomal location to Xp21. Xp21 fusion with 285 ribosomal RNA nucleus on chromosome 21, allowing marker XJ1.1 à closely linked to be isolated. 2) Use of DNA from a boy called ‘BB’ who suffered from 3 x-linked disorders: DMD, chronic granulomatous disease, retinitis pigmentosa. Genes responsible for these disorders are closely linked. Appeared that BB’s X chromosome cytogentically carried a visible deletion that affected part of all 3 genes. DNA by this deletion isolated from XXXXY cell line using substractive hybridization techniques. One of these clones, pERT87 closely linked to DMD mutation sites. pERT87 and XJ1.1 clones used to map locus constructing long-range restriction map. pERT used to probe cDNA libraries resulting in isolation of cDNA clones together spanned 14-kb mRNA of locus. Structure of the Lungs The lungs are located in the chest inside a lubricated membrane called the pleural membrane. - This allows the lungs to move freely inside the pleural cavity. The lungs are connected to the outside via the trachea (windpipe). The trachea is a tube kept in a rigid shape due to rings of cartilage. The larynx or voice box is located at the top of the trachea while at the bottom end it branches into two bronchi. These lead into the lungs. 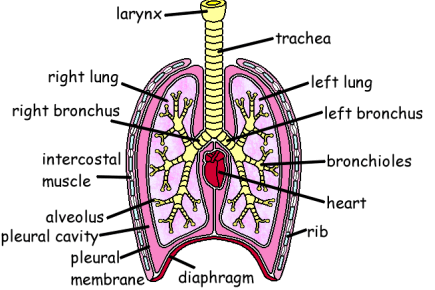 The bronchi in turn branch off into smaller and smaller bronchioles. These end in tiny air sacs called alveoli. It is here that gaseous exchange takes place. The surface area of all these alveoli is very large so as to be able to absorb oxygen very quickly. The lungs are very delicate and can easily be damaged. The cells lining the airways have very tiny hair like structures called cilia on them. These cilia are coated in a sticky mucus. The beating cilia force the mucus and any particles of dirt up out of the lungs. It eventually drops down into the oesophagus so the mucus is attacked by the stomach acid, destroying any pathogens. 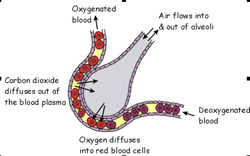 How We Breathe When we breathe, air is drawn into the lungs so that gaseous exchange can take place. The lungs are unable to draw in air on their own. The chest cavity where the lungs are positioned, is an air tight container. When we breathe in the diaphragm muscle contracts, pulling the sheet down. The intercostal muscles in between the ribs also contract which pulls the whole ribcage upwards and outwards. These together increase the volume of the chest. Air is drawn into the lungs because the the pressure inside them is lowered as the chest volume is increased. When we breathe out the diaphragm relaxes as does the intercostal muscles.This decreases the volume of the chest, increasing the pressure. This forces air out of the lungs. So it is the changing volume of the chest which causes air to enter and leave the lungs. The lungs themselves are just like balloons which are inflated and deflated. Gaseous Exchange The alveoli are the tiny air sacs at the ends of the bronchioles and the site of gaseous exchange. It is here that oxygen is absorbed into the blood while carbon dioxide is put into the air.  How We Breathe? When we breathe, air is drawn into the lungs so that gaseous exchange can take place. The lungs are unable to draw in air on their own. The chest cavity where the lungs are positioned, is an air tight container. When we breathe in the diaphragm muscle contracts, pulling the sheet down. The intercostal muscles in between the ribs also contract which pulls the whole ribcage upwards and outwards. These together increase the volume of the chest. Air is drawn into the lungs because the the pressure inside them is lowered as the chest volume is increased. When we breathe out the diaphragm relaxes as does the intercostal muscles.This decreases the volume of the chest, increasing the pressure. This forces air out of the lungs. So it is the changing volume of the chest which causes air to enter and leave the lungs. The lungs themselves are just like balloons which are inflated and deflated. Gaseous Exchange The alveoli are the tiny air sacs at the ends of the bronchioles and the site of gaseous exchange. It is here that oxygen is absorbed into the blood while carbon dioxide is put into the air.  Deoxygenated blood arrives at the alveoli in tiny blood capillaries. These have very thin walls, as does the alveoli itself. This makes it easier for the gases to pass from the air into the blood or vice versa. The deoxygenated blood has red blood cells low in oxygen and blood plasma high in carbon dioxide. The carbon dioxide diffuses from the blood plasma into the air. The oxygen diffuses from the air into the red blood cells. Blood constantly moves through the capillaries picking up O2 and giving up its CO2. Adaptations of Alveoli:
Smoking Smoking causes a number of diseases, some of them life threatening. To understand the effects of smoking you need to look at the components of cigarette smoke. Short Term Effects: Cilia can’t vibrate anymore, the air inhaled isn’t clean. Goblet cells release more mucus which makes the trachea narrower. Nicotine increases heart beat rate and blood pressure. Carbon monoxide combines with haemoglobin instead of oxygen combining with it. Carboxyhaemoglobin is formed which is stable. Less oxygen transported to cells. Diseases Caused By Tar: Chronic Bronchitis:
Lung Cancer:
Diseases Caused By Nicotine: This is the substance which makes smoking addictive. Nicotine is a stimulant which can make the heart beat faster and increase the amount of adrenaline released. It also makes the smoker more shaky. Increasing the normal heart beat rate can cause stress for the heart which can lead to heart disease. Coronary Heart Disease: Nicotine helps cholesterol deposition on walls of coronary arteries. This causes atheroma/atherosclerosis. Carbon monoxide also increases risk of blood clots forming which might results in blocking the artery. Less oxygen is delivered to cardiomyocytes (heart cells), a heart attack or failure can take place leading to death. Carbon Monoxide This is created due to incomplete burning of the tobacco. This gas binds irreversibly to the haemoglobin in red blood cells preventing them from carrying oxygen. This will make the smoker more out of breathe. If the smoker is pregnant then the amount of oxygen which is being passed on to the developing foetus is reduced. This slows down the growth of the foetus as it develops. 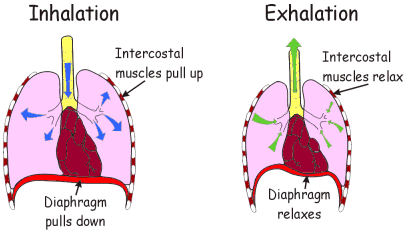 Thrombocytopenia is a platelet count that is under the normal lower limit (150 x 109/L). Platelets otherwise known as thrombocytes are located in the blood alongside red blood cells (erythrocytes), white blood cells (leukocytes) and plasma. The megakaryocytes are large cells that develop in bone marrow and undergo fragmentation to produce platelets. Platelets have no nucleus, instead they have granules where proteins are located to assist with its function. The function of platelets is to help with blood clotting. Platelets ‘stick’ together to stop the blood flowing from damaged blood vessels. This can be due to a number of causes: 1) Platelet function abnormalities: Thrombocytopathy – this can be due to defects such as genetics (inherited) and acquired of platelet function. Examples include Megakaryocytic hypoplasia – This is where megakaryocytes are underdeveloped, Wiskott-Aldrich syndrome (WAS) – This is an X-linked recessive disease. 2) Low platelet production. This can be due to disorders of bone marrow due to a number of reasons: Cancer: myeloma, leukaemia, lymphoma – It can also be caused by chemotherapy! Infection – mainly viruses such as HIV, hepatitis, Epstein-Barr, Cytomegalovirus, Herpes Simplex, Varicella-Zoster. 3) Low Platelet survival. This can be caused by: Immune This includes rheumatoid arthiritis, post-transfusion thrombocytopenic purpura (PTTP), neonatal alloimmune thrombocytopenia (NAIT). PTTP: This is where antigens on transfused platelets, destruct transfused platelets as well as the platelets of the patients. This normally occurs 10 days after transfusion and can last few weeks. NAIT: This is where the mother makes antibodies that are against the foetus (baby’s) platelets with paternal antigens. This can lead to severe neonatal thrombocytopenia. Drug-Induced Medications such as ibuprofen, vancomycin, heparin can cause thrombocytopenia. Pregnancy. In some pregnancies, HELLP syndrome can occur and stands for: · Haemolysis. · EL (elevated liver) enzymes. · LP (low platelet) count. 4) Dilutional thrombocytopenia This is caused by transfusion of high volumes of blood that may have dead platelets. Below is a diagnostic approach I created for thrombocytopenia and what tests recommended: In our blood, we have erythrocytes (red blood cells), platelets and leukocytes (white blood cells). All are made in the bone marrow. White blood cells protect the body from infections by ‘fighting’ them off. Platelets adhere together to stop bleeding by cover small cuts and in blood vessels. Red blood cells are disc-shaped and carry oxygen around our bodies and removes carbon dioxide from our bodies. Their normal lifespan is 120 days and then they die. The bone marrow in response produces more red blood cells for replacement. Haemolytic anaemia is where red blood cells are destructed and removed from the blood before their normal lifespan and the bone marrow cannot produce red blood cells rapidly enough to replace them. Thus, Haemolytic anaemia is a form of anaemia where there are a low number of red blood cells than normal. Anaemia is caused mainly by high rates of red blood cell destruction, lack of red blood cell production, loss of blood, lack of haemoglobin (iron-rich protein that carries oxygen around the body from the lungs) Haemolytic anaemia can lead to irregular heartbeats known as arrhythmias, heart failure, fatigue, enlarged heart and pain. Please find attached a diagnostic approach for haemolytic anaemia When is the Total Solar Eclipse? Friday 20th March 2015 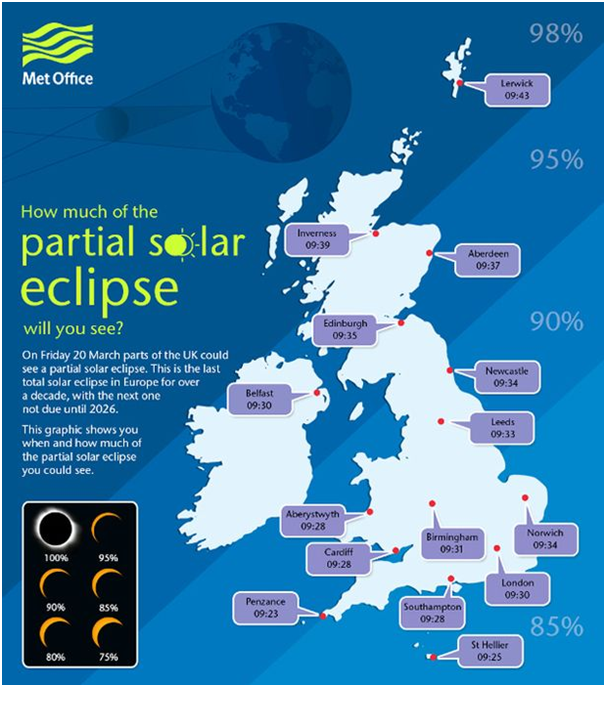  What is Solar Eclipse? There are three different types of Solar Eclipses. I will begin with the first type as that is what will occur if God wills on Friday. Total solar eclipses takes place when the Moon intervenes between the Sun and Earth and covers the Earth with its shadow. The shadow is called the umbra. The darkest phase looks like night. It consists of 5 phases: 1. Partial eclipse initiates: The Moon's shadow starts becoming visible over the Sun's disc. 2. Full eclipse initiates: Almost the entire disc of the Sun is covered by the Moon. 3. Total eclipse: The Moon completely covers the disc of the Sun. The Sky is dark, temperatures fall rapidly, and animals are quiet. 4. Full eclipse ends: The Moon's shadow starts moving away and the Sun reappears. 5. Partial eclipse ends: The Moon stops shadowing the Sun's disc. The eclipse ends.  Other types of eclipses include annular solar eclipse and partial solar eclipse. Annular solar eclipse is where the moon appears smaller than the sun and looks as though the sun has a bright ring surrounding the sun as shown below:
What effect can solar eclipse have on health? Generally, the eyes can be affected from intense sunlight due to the following:
In relation to the total solar eclipse, it is very dangerous to look at the sun directly during the solar eclipse despite it being covered fully by the Moon. No matter whether it was total, partial or annular eclipse – NEVER attempt to observe it with naked eye even if it was for a FEW seconds. This can lead to permanent eye damage especially to the retina. Eyes are very delicate ESPECIALLY children. Thus, more light are being transmitted to the retina due to higher sensitivity than the adult eye. This increases the risk to eye damage. Damage to the retina is known as solar retinitis/solar retinopathy. Mild damage may return to normal when the swelling at the retina is lowered. However, if there is severe damage, permanent damage can take place. Men are more at risk of solar retinopathy than women. NOTE: You will not be able to feel the effects of retinal damage as the retina has no sensitivity to pain. Amongst the symptoms that can be experienced are:
They can be experienced on both eyes (bilateral) but sometimes can affect one eye (unilateral). 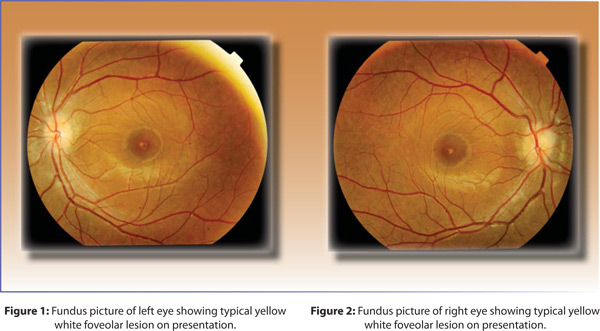  How can I protect myself? Safer techniques such as: 1) watching it via TV 2) using safe eyewear such as ‘eclipse glasses’. However, parents need to be cautious with their children who even wear such glasses. In addition due to limitations such as design, lens, improper use it is not advised to use such glasses. 3) Indirect contact such as projection method. Is it safe to drive during this time? There has never been a solar eclipse during ‘rush hour’. Thus there is a high chance drivers will be distracted by looking into the sky than focusing on what is happening on the road! Moving to the Islamic perspective of the solar eclipse. To show the power of Allah subhanahu wa taala, where none should worship only Him as He has the power to allow the moon to cover the sun and controls everything in the universe. He is the Almighty Allah subhanahu wa taala. ‘And among His Signs are the night and the day, the sun and the moon. Prostrate neither to the sun nor to the moon, but prostrate to Allah who created them, if it is truly Him you worship.’ (Surah Al-Fussilat 41:37) Solar eclipses are reminders of the Day of Judgement where the moon, sun and stars lose lights. ‘When the sight is dazed, and the moon is buried in darkness, and the sun and moon are joined together: Man will say on that day, ‘Where is the refuge?’’ (Surah Al-Qiyamah 75: 7-10) What do Muslims do during the solar eclipse? During the Eclipse, Muslims pray the Salah al-Kusoof (The Solar Eclipse Prayer). Please do not get mixed up with Salah Al-Khusoof (Lunar Eclipse). Both do contain to Rak’aat (units of prayer). Majority of the people of knowledge confirm it to be a sunnah mu’akkadah. Imam Malik compared its importance to that of the Friday Prayer whereas Imam Abu Hanifah confirmed it to be obligatory. It is sunnah to pray at the masjid in congregation. However, those who are unable to do so may pray alone. Women can pray at home or pray in congregation. What does Salah Al-Kusoof consists of: The prayer lasts throughout eclipse. The sermon is delivered after the Prayer. Recitation is performed loud. There are two Ruku‘s (bowing), the second of which is always shorter than the first, and there are also two recitations. After the Takbirat-ul-Ihram (saying: “Allahu Akbar [Allah is the Greatest]” upon starting Prayer), Surah Al-Fatihah and a long Surah are recited. After the first Ruku‘, Surah Al-Fatihah and a long Surah are recited, which is shorter than the preceding recitation. There are two Sujuds (Prostrations) in each Rak‘ah. This is the most authentic report mentioned regarding this Salah. [Source: Sh. 'Abdul-`Aziz ibn `Abdullah ibn Baz; alifta.net] Urwah bin Az-Zubair may Allah be pleased with him reported from Aishah may Allah be pleased with her, the wife of The Prophet peace be upon him, that she said: “There was a solar eclipse during the lifetime of Allah’s Messenger peace be upon him. So, The Prophet peace be upon him went to the Masjid, stood up and said the Takbir, and the people lined up (in rows) behind him. Allah’s Messenger peace be upon him recited (the Qur’an) for a long time, then said the Takbir and went into Ruku’ for a long time. Then he raised his head & said: ‘Sami Allahu liman hamidah, Rabbana wa lakal Hamd.’ So he stood up and recited a lengthy recitation, which was not as long as the first recitation. Then he said the Takbir and went into Ruku’ for a long time, but not as lengthy as the first Ruku’. Then he said: ‘Sami Allahu liman hamidah,’ and he repeated the same acts in the other raka’at. So he completed four Ruku’ and four prostrations (Sujood), and the sun had become visible before he finished.” [Source: Hadith No. 1180, Book of The Prayer for Rain, Sunan Abu Dawud, Vol. 2].  |
A GOOD HEALTH MAKES YOU RICHHealth is crucial in every single person’s life. Its something that money can’t buy. Thus a good health makes you rich so look after it. Archives
May 2017
Categories |
Welcome

 RSS Feed
RSS Feed
© COPYRIGHT 2013. ALL RIGHTS RESERVED.
Proudly powered by Weebly