 My journey in understanding how the anatomy and physiology of the human body with the Glorious Quran interconnects continues. This is associated with Tawassum (ability to understand) where I am inspired to observe and reflect on nature which provides us with a meaningful purpose and spiritual nourishment. Allah (The Most High) says: “Indeed in that are signs for those who discern.” [Quran, Surah Al Hijr, 15:75] The ability for us to reflect and analyse is known as Tadabbur and is derived from ‘dabara' or ‘dubr' meaning back (Chaudhary, 2020). When we observe the face of someone, we do not look at their back nor effort that is deepened. Thus, if we want to understand the Glorious Quran, we need to deepen our exploration of divine speech of Allah (The Most High) (Chaudhary, 2020). Therefore, there is a potential benefit through Taffakur (thinking) and Taddabur (reflection) that function in an integrated matter. Allah (The Most High) states: “Do they not reflect on the Qur’an carefully (yatadabbarun al-Qur’an)?” [Quran, Surah an-Nisa’, 4:82] In another verse, Allah (The Most High) states: “We created man of the best stature (mould)” [Quran, Surah At-Tin, 95:4]. Allah (The Most High) has created humankind in the best form and amongst the anatomical details found in the Glorious Quran is the human senses that gives us the power to perceive the world around us. However, it must be emphasized that is the All-Powerful and He alone is in control of all things. Allah states in the Quran: "It is Allah who has created seven heavens and of the earth, the like of them. [His] command descends among them so you may know that Allah is over all things competent and that Allah has encompassed all things in knowledge." [Quran, Surah Talaq, 65:12] Human senses can be divided into internal and external senses that collaborate to assist with our health and well-being (Sempo et al. 2017). Internal senses are associated with feelings and emotion, for instance, happiness, gratefulness, sadness and anger. Thus, our internal senses are associated with our psychology on three levels: sub-personal, behavioural and phenomenal (Fulkerson, 2014). On the other hand, external senses are linked to the sensory system that consists of special sense organs that detect excitatory information from the environment (Knight, 2017). This is then relayed to the brain in the central nervous system to process into sensations via neural pathways (Gadhvi and Waseem, 2020). Our body contains a five-sense device, eyes to provide us with vision, olfaction via our nose, the ability to hear with our ears, taste (gustation) with our mouths, touch (tactile perception) with our hands and somatic sensation (Ibn Sina, 1952a; Sempo et al. 2017; Knight, 2017). Thus, the anatomy and physiology of the human senses are vital in understanding the different sensations (Gadhvi and Waseem, 2020). Dysfunctional effects of these modalities would decrease our ability to communicate and understand the world around us and; the diminished acuity will increase as we age (Knight, 2017). One of the dysfunction effects of the sensory system is cancer where there are side-effects of patients undertaking radiotherapy and chemotherapy (McWilliams, 2008). Patients with cancer lose their ability to taste and smell due to the cancer therapies administered that can dysfunction the olfactory and taste receptor cells causing morphological changes and dysgeusia ( slight change in taste) to complete change in taste (aguesia) for sweet, sours, bitter and umami food flavouring and can also affect the peripheral system (Altundag and Cayonu, 2016, McWilliams, 2008). Statistics have shown that there is a ca. 77% chance cancer patients have this symptom of an infrequent smell and is common amongst patients with head and neck cancer (Altundag and Cayonu, 2016). Besides, metabolic changes can also occur. Other diseases in response to dysfunctional effects of the sensory system include fungal infections, for instance, dry mouth, ulcers, thrush (Schiffman, 2007). Deficiencies, for instance, Vitamin A, niacin is associated with cancer (Rehwaldt et al. 2009) Allah (The Most High) states: “And Allah has extracted you from the wombs of your mothers not knowing a thing, and He made for you hearing and vision and intellect that perhaps you would be grateful” [Quran, Surah Nahl, 16:78] Furthermore, Al-Nahlawi (1983) informed that the heart has other functions besides pumping oxygenated blood around the body to provide nutrients for cells, tissues and organs. The heart provides thoughts, for instance, happiness and gratefulness and the ability to observe and visualise the development of science via assessment and results. This suggests that the human senses are fundamental in creating environmental sustainability and is embedded in the Quran and Sunnah and protected by the Maqaseed Al Shariah otherwise known as ‘The Objectives of Islamic Law' (Asmawati et al. 2020). There are two forms of Tafsir: Tafsir Al Maatoor (Traditional explanation) and Tafsir bil Al ra'yi (explanation with reason) and this can be achieved with our senses that have a vital function to shape our knowledge, understanding and contribution (Abbas, 1973; Asmawati et al. 2020). Ibn Qayyim (2018) mentioned that our human senses are blessings and will testify against us on the Day of Judgement where Allah has stated in the following verses: “This Day, We shall seal up their mouths, and their hands will speak to Us, and their legs will bear witness to what they used to earn.” [Quran, Surah Ya-Sin, 36:65] “On the Day when their tongues, their hands, and their legs or feet will bear witness against them as to what they used to do. [Quran, Surah An-Nur, 24:24]. This emphasises how our human senses correlate with our faith where we listen to the Fardh (mandatory) and the Sunnah and avoid what is prohibited (Ibn Qayyim, 1991). For instance, we listen to the Quran, a lecture or a halaqa and avoid things that affect the heart and idle speech. The process of how our human senses function Our body consists of specialised cells called receptors that receive the stimuli and translate it into signals. There are various forms of receptors summarised in Table 1. Examples of the somatovisceral receptors include mechanoreceptors for touch, thermoreception due to the alteration of the hot and cold weather and pain (nociception) to regulate homeostasis, blood pressure and respiratory rate (Gebhart, 1995). Table 1: The various types of receptors 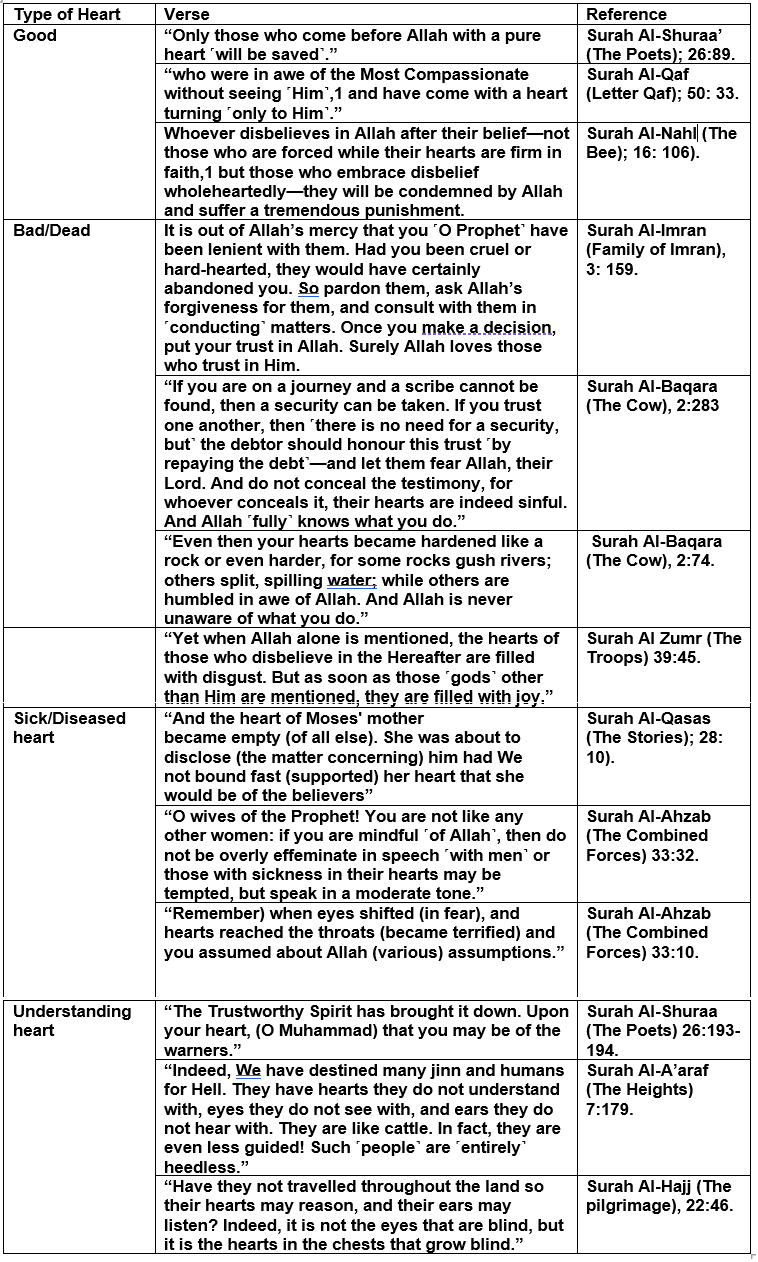 There are three types of nerves otherwise, known as neurones presented in Figure 1. Their structures vary but they all have dendrites to receive signals and connect with the cell body. Axon facilitates action potential (Catala and Kubris, 2010). The myelin sheath insulates the axon and, the axon terminal connects neurons via a synaptic transmission (Allen and Schwartz, 1940). 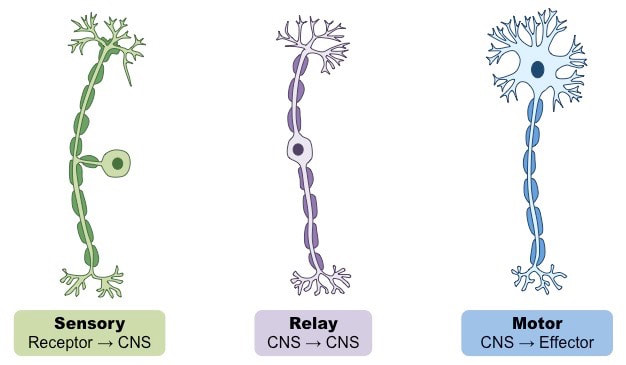 Figure 1: The three types of neurons The signal is transmitted as action potential via the sensory neuron from the dorsal ganglion root in the peripheral nervous system where it is then converted to electrochemical energy in the sensory cortex in the spinal cord (Allen and Schwartz, 1940). The central nervous system consists of the brain and spinal cord. This is known as transduction. The sensory neuron is of a pseudounipolar sub-type where it has no dendrites. The peripheral branch extends from the cell body to the skin, joints and muscles, whereas, the central branch extends from the cell body to the spinal cord (van Stralen and Dijikerman, 2017). There are two pathways in how sensory neurons transmits the nerve impulses to the spinal cord that conveys somatosensory input as illustrated in Figure 2. Spinothalamic pathway comprises of pain, touch, temperature and sensations to several thalamic nuclei (Allen and Schwartz, 1940; Irvine and Clark, 2017; van Stralen and Dijikerman, 2017). The second pathway is the dorsal column which is required for touch, vibrations and proprioception (Ghanty and Schragg, 2019). 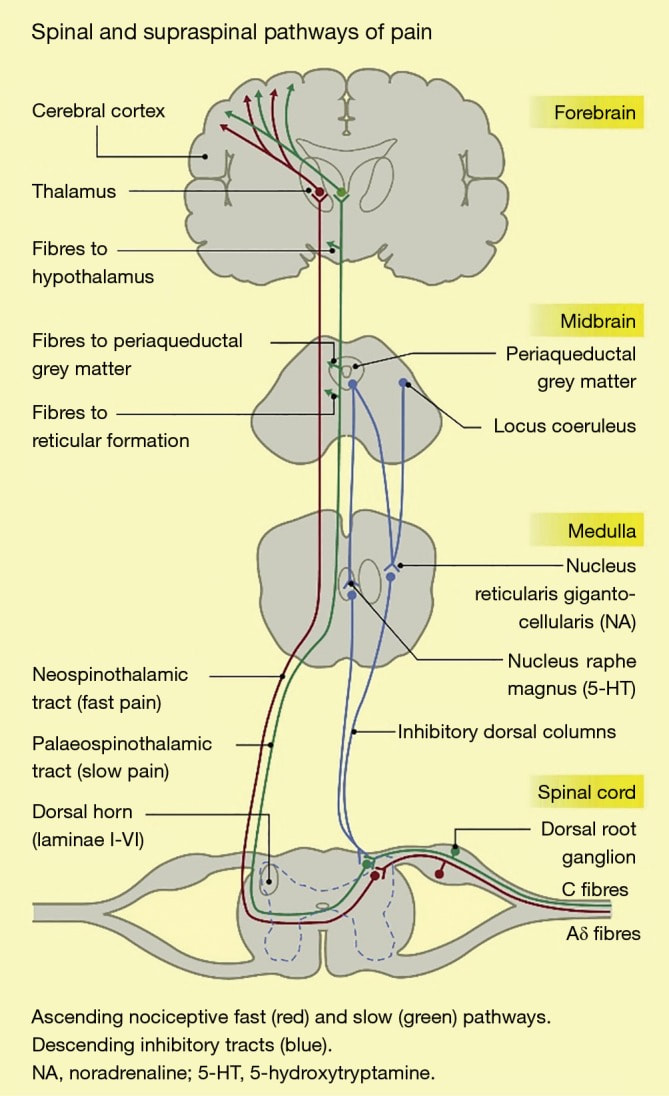 Figure 2: The neural pathways: supraspinal and dorsal column (Ghanty and Schraag, 2019) For example, for hearing to occur, the hair cells of the auditory system act as receptor cells cause the stereocilia to bend. There is an energy transfer from mechanical energy to electrochemical energy in response to the flow of ions via channels into the membrane to generate cell membrane potentials which could be depolarization or excitation (Hudspeth and Gillespie, 1994). The intensity of the potential depends on the time, rate and strength of the stimulus. There is a constant force in the bending of the stereocilia. The mechanical mechanism is stimulated by the proteins actin and myosin to reset the tension and transduction to the resting state where the sensory cell can respond to new stimuli (Hudspeth and Gillespie, 1994; Sokolowski 2007). Upon the signal reaching the central nervous system, the relay neurons allow the sensory neurones and motor neurons to communicate (Bishop, 1980). The fibres are classified based upon sensation, size of diameter and velocity (Catala and Kubris, 1980). The classification is known as Erlanger Gasser and consists of four groups: Group 1 alpha are fibres from the primary endings of muscle spindles. Group 1 beta is from Golgi tendons. Group 2 beta is from secondary endings of muscle spindles as well as touch receptors in the skin. Group 3 delta is from muscle endings and skin. Group 4 are from the skin and muscles (Dubin and Patapoutian, 2010). The motor neurones function in controlling muscle movements where it releases neurotransmitters that associate with the receptors in muscles (Catala and Kubris, 2010). Therefore, the sensory system and the central nervous system is vital to interconnect to produce a response. The power of hearing Hearing is one of the human senses that has been created by Allah (The Most High) before vision in the foetus where he or she can hear the voice of the mother whilst it is in the womb. We have been blessed with a pair of ears to function in hearing, listening, communication, balance, consciousness and alertness. The Glorious Quran has various evidence of its physiological purpose. “We created man from a fertilizing sperm, to test him; and We made him hearing and seeing” [Quran, Surah Insaan, 76:2] "Why are its verses not explained in detail [in our language]? Is it a foreign [recitation] and an Arab [messenger]?" Say, "It is, for those who believe, a guidance and cure." And those who do not believe - in their ears is deafness, and it is upon them blindness. Those are being called from a distant place.” [Quran, Surah Fussilat, 41:44] “ It is He who produced for you the hearing, and the eyesight, and the feelings. But little gratitude you show “And if We had made it a non-Arabic Qur'an, they would have said” [Quran, Surah Muminoon, 23:78] “Do they have feet by which they walk? Or do they have hands by which they strike? Or do they have eyes by which they see? Or do they have ears by which they hear? Say, [O Muhammad], “Call your ‘partners’ and then conspire against me and give me no respite.” [Quran, Surah Haqqah, 69:12] The ear is divided into the outer, middle and inner ear as presented in Figure 3. The ears alter the vibrations perceived as sound where the outer ear consists of the pinna and the external auditory ear canal. The pinna is made of cartilage and gains high-frequency sound waves where they are funneled down the ear canal that acts as a resonating tube and protective barrier to the tympanic membrane. The ear canal consists of the sweat gland and oily sebaceous glands that together form earwax (Alper et al. 2017). The tympanic membrane is also known as the eardrum is a thin membrane that associates with the Eustachian and mastoid air cells (Alper et al. 2017). It forms part of human auditory apparatus (Alper et al. 2017). A perforated eardrum can cause hearing loss (Mayo clinic, 2020). This is why Allah says in the Quran: "Among them are those who listen to you; but We place covers over their hearts, to prevent them from understanding it, and tear in their ears. Even if they see every sign, they will not believe in it. Until, when they come to you, to argue with you, those who disbelieve will say."This is not but legends of the former peoples." [Quran, Surah Al-Anaam 6:25] The middle ear is where mechanical vibrations can be heard in the membrane. Most sounds are transmitted by air to cause vibration, however poor vibration occurs where two areas differ in the density and speed of sound such as water. The eustachian tube (pharyngotympanic tube) ensures the pressure in the middle ear is balanced with the pressure in the atmosphere. The vestibular complex in the inner ear also facilitates and is based on receptors that sense equality. The middle ear extends from the air passages of the nose and sinus lining the respiratory membrane. It absorbs the gases, carbon dioxide and oxygen from the air in the middle of the ear and; this may produce pain. The back end of the nose in the nasopharynx consists of cartilage and muscle (Alper et al. 2017). The tympanic membrane transfers the mechanical vibrations to auditory ossicles. Auditory ossicles are three small bones found in the air cavity of the middle ear: malleus (hammer), incus (anvil) and stapes (stirrup) (Richardson et al. 1939). The stapes bone pushes the oval window in and out the vibrations to the spiral-shaped organ of Corti otherwise known as the cochlea. They transfer the vibrations to the inner ears (Alberti, 2005). The vibrations are transduced by the cochlea to the perilymph via the ossicular chain into a nerve impulse by the delicate hair cells that detect pressure in the fluid cavity where receptors are activated and; is carried along the statico-acoustic nerve/ vestibulocochlear nerve from the cochlea to be processed in the brain via the auditory pathways to produce sound (Alberti, 2005; Richardson et al. 1939). The nerve fibres split where they pass one side of the brain and; the rest remain unchanged because they ascend to the hindbrain to the midbrain and the cerebral cortex (Alberti, 2005). This highlights the auditory function of the ears and its role in balance. 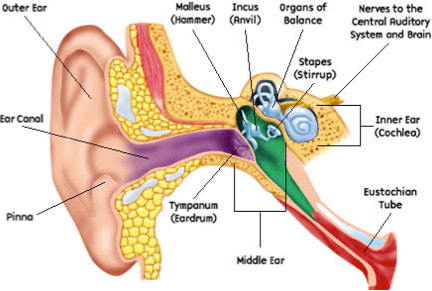 Figure 3: The structure of the ear (Shannon, 2010). The power of vision We initiate in the wombs of our mothers without vision and then blessed with the visual tool, our two eyes, following the development of the primitive features of our ears. The primary function of the eyes is to perceive the outside world where we can capture, adjust and transform the size, colour (stereopsis), type and length of the distance of what we see via neuroreceptors. This is based upon the light patterns where it can either reflect, refract, diffract, dilate or constrict (Zhu et al. 2012). “And Allah has extracted you from the wombs of your mothers not knowing a thing, and He made for you hearing and vision and intellect that perhaps you would be grateful” [Quran, Surah Nahl, 16:78] To be able to thank Allah (The Most High) for this blessing would be insufficient. Allah is Our Inventor. Our Creator. Our eyes are also the door to the aperture of our hearts; hence it contains vivid information of our emotions and well-being. It allows us to be aware of trials and become more conscious. Ibn Al-Qayyim (1991) stated: “Contained within the crystal is a lamp, and it is the light which is in the wick – and it is its carrier, and for that light, there is an ingredient – and it is oil which has been pressed out of an olive that originates from the most equitable of places. The sun gleams upon it at the first portion of the day as well as its latter; hence its oil is from the clearest of oils and the furthest of them from cloudiness, such that due to its clarity it virtually illuminates without flame – this is the ingredient of the light of the lamp. Likewise is the ingredient of the light of the lamp which is in the heart of the believer, it is derived from the tree of revelation which is from the greatest of factors for blessing – and the furthest of them from misguidance.” Allah (The Most High) states: “So have they not travelled through the earth and have hearts by which to reason and ears by which to hear? For indeed, it is not eyes that are blinded, but blinded are the hearts which are within the breasts.” [Quran, Surah Al-Haj, 22:46] This highlights the importance of our heart and its natural connection with the eyes from a spiritual and physical context. From the spiritual perspective, Allah looks into the quality of our hearts whereby intention, knowledge, belief and relationship are key factors to determine the viability of the heart, for if the stated elements are sound, the heart will not be diseased. On the other hand, our eyes also reveal pathological features that relate to our heart. Tiny, blood vessels in the eyes called the retinal vasculature associate with the heart. High blood pressure or hypertension can cause visual damage due to the significant pressure within the blood vessels. This can lead to blurry vision, blood clots and bleeding in the eyes. Besides, it can also lead to strokes hence why an eye examination takes place to investigate the presence of constriction to blood vessels, spots and swelling. The anatomical features of our eyes The human eye has three layers: outer, middle and inner layers as presented in Figure 4. The outer layer consists of the sclera and cornea. The middle layer comprises of the choroid, iris and the ciliary body. The inner layer contains the retina. The distinctive features of the eye together allow the focusing of the images on the retina to exert their regulatory functions of the light, protection, motion and provide nutrition. The complexity of the eyes and the nerve fibres that associate the eyes with the central nervous system cannot be transplanted nor reconstructed. This further highlights the extent of the engineering skills that Allah (The Most High) possess. For He is All-Seeing. All-Aware, The inventor and the Creator. “Vision comprehends Him not, but He comprehends (all) vision. He is the Subtle, the Aware. Insights have certainly come to you from your Sustainer; then whoever sights, does so for his own self, and whoever is blinded, does the same. And (say): I am not over you an overseer.” [Quran, Surah Al Anaam, 6:103-104] 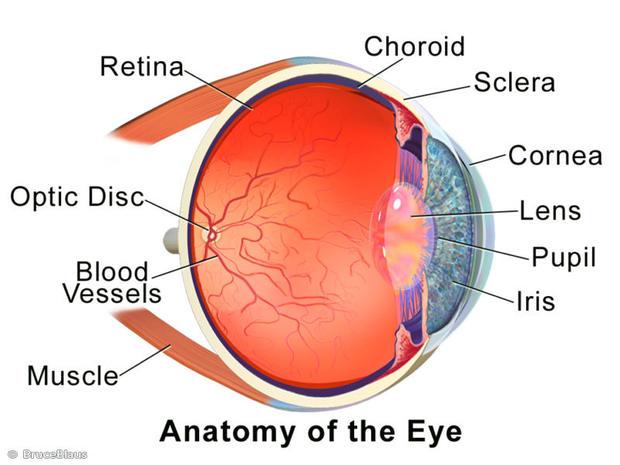 Figure 4 The structure of the eye (Blaus, 2020) Amongst the features in the outer layer is the cornea, a clear, transparent and dense layer with a horizontal and vertical diameter, 11.5 mm and 10.5 mm respectively (Muller et al., 2003; Farjo et al., 2009). It refracts and transmits light to the pupil, lens and retina (Muller et al. 2003). It also protects the eyes from trauma, damage and infection (Van Burskirk, 1989). Most of the corneal nerves are sensory nerves derived from the ophthalmic branch of the trigeminal nerve (Muller et al. 2003; Farjo et al. , 2009). The cornea is situated in the anterior area of the fibrous tunic which is presented in front of the iris and pupil and consists of four distinctive sub-layers: Corneal epithelium, Bowman's membrane, Corneal stroma, Descemet's membrane and Corneal endothelium (Van Buskirk, 1989). The Corneal epithelium has an impermeable and stable basement membrane comprising of several layers of wing cells and one basal cell layer due to the cell junctions (McCaa, 1982). The Bowman's membrane is a clear and homogenous layer. The collagenous feature of the corneal stroma maintains the mechanical strength, structural integrity and diptropic stability of the cornea and forms 90% of the cornea (Van Burskirk, 1989). The stromal keratocytes secrete the collagen and proteoglycans. Proteoglycans regulate the hydration level where the fluid flux from the stroma produces water required for transparency; deturgence (McCaa, 1982; Muller et al. 2003). The Descemet's membrane is a strong, homogeneous basement membrane. It consists of endothelial cells that provide an elastic feature and; this thickens with age where the anterior end is banded and; the posterior ending is amorphous (Zhu et al. 2012). The Corneal endothelium has a single cell layer containing flat, cuboidal cells that maintain the dehydration of the corneal tissue. Destruction to the structure of the endothelium can cause swelling and loss of transparency of the cornea (McCaa, 1982). The sclera is a white, opaque connective tissue situated in the posterior end of the tunic (Willoughby et al. 2010). Its function is to maintain the shape of the eye and protect the internal structures from damage. It is covered by a transparent, mucous membrane called the conjunctiva (McCaa, 1982). The iris is the coloured area of the eye situated in the middle ocular layer. It acts as a window shutter or a diaphragm where it has an involuntary control in the size of the pupil and the amount of light that enters the retina (McCaa, 1982). The autonomic nervous system consists of the sympathetic and parasympathetic nervous system. The sympathetic system has a fight or flight response where it responds to fear, bright light causing the radially oriented pupillary dilator muscle to contract in the iris which results in the dilation of the pupil (mydriasis). Similarly, the nervous system responds dramatically when the astronauts travel to space. Amongst the symptoms felt is dizziness and nausea during the initial days and; this progresses to the blurred vision that corresponds to symptoms when drunk. Allah (The Most High) says: “And [even] if We opened to them a gate from the heaven and they continued therein to ascend, They would say, "Our eyes have only been dazzled. Rather, we are people affected by magic." [Quran, Surah Al Hijr, 15, 14-15] The parasympathetic nervous system has a rest or digest response where it conserves energy for sleep, digestion and seeing during dim light where the pupil constricts (miosis). The scholars such as Ibn Amir Al-Hajj (May Allah have mercy upon him) states: “Sleep is a state that occurs to the intellect that necessitates the incapacity of a person to perceive sensory things, to conduct involuntary actions, and the general use of the intellect.” (Dar Al Ifta, 2020). Another feature found in the middle layer is the uvea. The uvea provides nutrients where the posterior end is the choroid and; the other area of the uvea is called the ciliary body (Schubert, 2009). The choroid is a vascular layer that consists of blood vessels that provide oxygen and nutrients to the outer retinal layers. On the other hand, the ciliary body produces intraocular fluid known as the aqueous humour. Additional roles of the ciliary body are to provide muscle support, control the shape and power of the lens (McCaa, 1982). The lens is situated behind the iris and is supported by a suspensory ligament; the zonule (McCaa, 1982). Behind the lens is a vitreous gel that occurs between lens and retina (McCaa, 1982). The retina is situated in the inner layer surrounding by the dura mater; a dense fibrous tissue. It is a complex, delicate membrane of neurones and is protected by the sclera and cornea (Schubert, 2009; Masland, 1986). There are various types of neurones present in the retina: bipolar, photoreceptors, amacrine, ganglion cells, horizontal cell and Mullerian glia. The photoreceptor, bipolar, horizontal, amacrine and ganglion process whereas the glial cells organise the back of the retina (McCaa, 1982). There are two types of photoreceptor cells: rods and cones. The cones translate light into colours and vision and have pigments with a high absorption peak in the blue and green spectrum (McCaa, 1982). The rods translate the light into peripheral vision and motion and have low light levels (McCaa, 1982). However, this is dependent on several factors, for instance, the wavelength, the intensity of the light and the area illuminated. The macula lutea in the retina comprises of xanthophylls pigment and several ganglion cells. Within the macula, the fovea has high levels of cones required for central vision; whereas the lower end of the fovea contains dense cones and is known as the foveola. The density of the foveola allows the synaptic terminals and the ganglion cells to the centre where Henle's fibres are formed between the nuclei and synaptic terminals (McCaa 1982). The retinal pigment epithelium (RPE) is arranged in a hexagonal format and; the pigment granules are found in the apical end of the RPE where lipofuscin and melanin are produced (McCaa, 1982). RPE consists of two blood-retinal barriers: retinal and the choroid where the former supplies the inner retina whereas; the latter received from the choroid circulation via diffusion. Additional roles of the RPE include pigment formation, adhesion, production of growth factors, wound healing and metabolism of Vitamin A (McCaa, 1982). The visual pathway - how can we see? The photoreceptor cells capture the image in the back of the retina. It is inverted as it progresses through the lens where there are two optic tracts. The left optic tract has half of the image projected onto the nasal retina of the right eye and the temporal retinal of the left eye. On the other hand, the right optic tract has a left image projected onto the temporal retinal of the right eye and the nasal retina of the left eye. This is processed and converted to nerve impulses or electrical signals (phototransduction). The signal passes from the axon of the ganglion to the optic disc and then the second cranial nerve called the optic nerve (Willoughby et al. 2010). The optic nerves from each eye produce the optic chiasm where the fibres from the nasal retina travel to contralateral optic tract; whereas the fibres from temporal retina remain ipsilateral (McCaa, 1982). The is presented in Figure 5. The optic tract travels to the specific cerebral hemisphere to the lateral geniculate nuclei (LGN). The LGN is situated in the thalamus and consists of neurons that send axons to the ipsilateral primary visual cortex via fibres radiation to process the sensory information. There are two types of optic radiation: the upper optic radiation transfers the fibres signal to the cortex via the parietal globe whereas the lower optic radiation achieves this via the temporal lobe and this is called Meyer's loop (Schubert, 2009; Masland, 1986). Upper optic radiation carries fibres signal to the parietal globe to reach the cortex. Lower optic radiation carries fibres via temporal lobe and; this is called Meyer's loop to reach the visual cortex. Once at the cortex, it will process sensory information (Schubert, 2009). The horizontal and amacrine cells modify and control signal. Allah says in the Quran: “Have We not made for him two eyes?” [Quran, Surah Balad, 90:8] 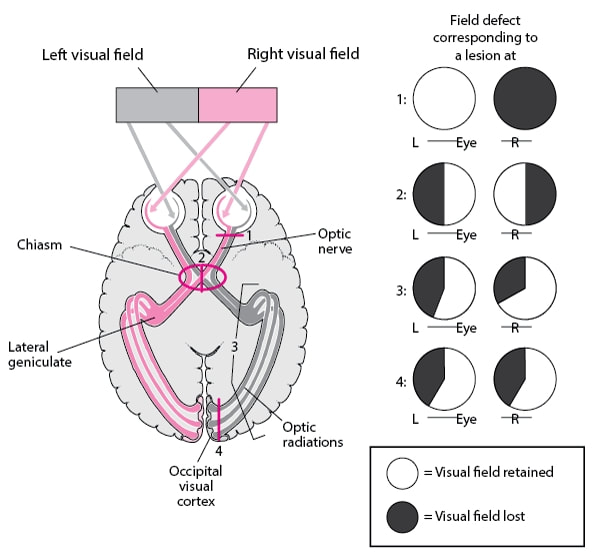 Figure 5: The visual pathway (Garrity, 2020) The power of smelling The function of the nose is to provide an exchange of the air between the environment internally and externally where oxygen is inhaled and; carbon dioxide is exhaled (Jones, 2001). The anatomical structure and function of the nose and paranasal sinuses are fundamental for olfaction, the modification and transformation of inspired air towards 38 oC and 100% relative humidity (Proctor and Adams, 2008; Guerkink, 1983). Inside the nose, there are two cavities: nasal cavity and paranasal in the centre of the face and are also found in the skull (Jones, 2001; Proctor and Adams, 2008; Sahin-Yilmaz and Naclerio, 2011). The left and right nasal cavity (choanae) is divided by a middle wall called a septum. The septum is composed of cartilage (anterior) and bone (posterior) that together aid in increasing the mucosal surface area (Sahin-Yilmaz and Naclerio, 2011). At the bottom of the nasal cavity, there is a floor which extends to the back where it associates with the nasopharynx. The nasopharynx is at the back of the throat and interconnects the nasal cavity with the oropharynx. On the side of the nasal wall are little projections called turbinates (conchae) as presented in Figure 6. They contain cancellous bone made with trabeculae surrounded by respiratory epithelium and function in increasing the mucosal surface between the range 100cm to 200 cm to filter and humidify the air (Sahin-Yilmaz and Naclerio, 2011). There are three types of turbinates: inferior (lower), middle, superior (upper) and sometimes a fourth one called supreme. 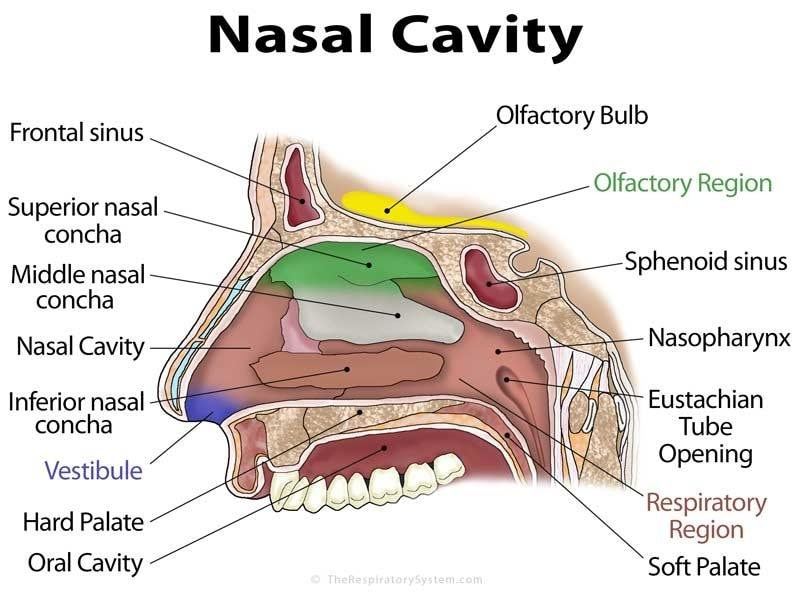 Figure 6: The anatomical features of the nose (Sabale et al. 2020) Sinuses produce mucus to moisturize the nasal cavity, humidify the air, lighten the weight of the head, protect the skull from damage and allows a resonating voice to occur (Thanc Foundation, 2020). There are four main types of sinuses: maxillary, ethmoid, frontal and sphenoid sinuses. Maxillary sinuses are found in the cheek and contain mucus to drain into the nasal cavity under the middle turbinate. This commonly where sinonasal cancer arises from. Ethmoid sinuses are composed of 10 to 20 small sinuses that have thin walls and; the mucus is extracted under the middle and superior turbinates (Sahin-Yilmaz and Naclerio, 2011). The frontal sinuses are situated in the forehead and drain the mucus from the nasal cavity below the middle turbinate to a passage called the nasofrontal duct. Sphenoid sinus resides at the base behind the nose below the superior turbinate. Besides, there is a tear duct that drains the tears from the eyes under the inferior turbinate (Sahin-Yilmaz and Naclerio, 2011). Allah states: “We will brand him upon the snout" [Quran, Surah Al Qalam, 68:15]. Outside the nose, various cartilages are supported by the septum, for instance, the lateral (alar) has two at the top and two at the bottom. The lower lateral consist of medial and lateral cruca. The small muscles: nasalis, deptessor septinasi, levator labii superioris alaquei asi lower the nasal resistance and dilate the nostrils (vestibule) (Dion et al. 1978). Vestibule consists of stratified epithelium. The anterior nasal glands secrete the serous mucus and; this is where sniffing occurs that causes the stimulation of secretions. Humans have various types of receptors where the neuron in the olfactory cleft situates in the nasal cavity near the olfactory bulb and fossa. Amongst them are thermoreceptors who upon stimulation cause a nasal resistance in the airway. However, during inspiration, the warm air decreases the nasal resistance where there is ca. 50-75% resistance from ambient air to the pulmonary alveoli whereas, in the cold air there is an increase in the nasal resistance where there is more time for gas exchange in the alveoli and the air is more turbulent. This causes the inspired air to interact with the nasal mucosa and warmed as it reaches the nasopharynx (Connel and Fregosi, 1993; Cauna 1982). Posterior to the vestibule is the nasal valve where the dilator naris muscle increases the surface area and airflow from 40 to 150 mm squared (Sahin-Yilmaz and Naclerio, 2011). Al-Qastallani writes: “Let him sniff water three times to expel harmful things after he blows it out from his nose, for it cleans the airways through which the Quran is recited.” [Irshad Al Sari] Upon smelling, the sense receptors associate with the chemicals present in the air in the olfactory cleft transmit the smell to the brain via the hair-like cilial structures in the epithelium in the upper nasal cavity (Sahin-Yilmaz and Naclerio, 2011). They travel to the olfactory bulb that contains neurone cell bodies that transmit the peripheral information along the cranial nerves. This transcends to the olfactory nerves to the olfactory cortex in the cerebral cortex of the brain (Sahin-Yilmaz and Naclerio, 2011). They will then process all information about the intensity, hedonics and memory of the odour. Therefore, this amazing structure that is situated between the eyes has a prominent function where it is an olfactory organ and also is a doorway to the respiratory tract where it can sustain 20 to 30 L of airflow per minute and; if a higher volume of air is needed, a combination between oral and nasal breathing occurs (Sahin-Yilmaz and Naclerio, 2011). The power of tasting The oral cavity or the mouth is the space that initiates from the upper lip to the hard palate and consists of teeth, mandible, hard palate, buccal and gingival mucosa, floor, tongue and the circumvallate papilla as presented in Figure 7 (Cohen, 2013). The mouth has a gustatory sense for various tastes of what we consume by the presence of buds. In total, there are ca. 2,000 to 4,000 taste buds where the majority of buds reside on the tongue, the remainder can be found in the nasal cavity, oesophagus, epiglottis and the back of the throat (InformedHealth.org, 2016). Allah (The Most High) states: ‘And a tongue and two lips?’ [Quran, Surah Balad, 90:9] The taste papillae under the mucous membrane of the tongue have taste buds. There are different types of taste papillae: fungiform papillae, circumvallate papillae and foliate papillae. Fungiform papillae contain 200 – 400 sensory cells on the surface of the tongue on the tip and near the edge. They also have sensory cells for touch and temperature. Circumvallate papillae are at the base of the tongue and have V-shaped sensory cells. Foliate papillae are on the rear edges where there are around 20 with a few hundred taste buds in each (InformedHealth.org, 2016). The gustatory/sensory cells in the taste buds are connected to nerve fibres and form flower-shaped capsules that have a fluid-filled funnel containing finger-like projections called taste hairs (InformedHealth.org, 2016). The proteins on the surface of the hair fuse with chemicals for tasting. Amongst the taste buds are sour, sweet, salty, bitter and; umami (InformedHealth.org, 2016). The remainder of the taste buds function in the intensity of the taste, for instance, how sweet or sour something is. Many assume that spicy is also deemed as a taste but is classified as a pain signal. The sensation of sweetness is caused by the presence of fructose and lactose and other derivatives that activate sensory cells. Food that has acidic solutions, for instance, lemon juice and organic acids contain hydrogen ions dissolved in aqueous solution. The savoury taste can be described as meat broth by the presence of glutamic or aspartic acid. The mineral salts of potassium, sodium and magnesium enable the sensation of saltiness to occur. This is a similar case with bitter food that provide a bitter sensation (InformedHealth.org, 2016). The teeth help to grind the food and spread the aroma around the mouth. Cleaning the teeth is part of health and well-being. It has been advised that during the following five scenarios it is mustahabb (recommended): when the teeth are yellow, the breath of mouth changes, when waking up, praying and performing ablution (Ibn Abidin, 1979). The Prophet (peace be upon him) used a wooden stick called miswak to clean the mouth during the morning and night. Some were unsure of how many times he utilized it (Omar and Ibn Hanbal' 2004). He said in a hadith: Prophet Muhammad (peace be upon him) said: “Use miswak. Certainly, miswak is a cleansing for the mouth.” [Bukhari, Nasai', Ibn Majah] Today, many observe this as part of Sunnah and; we are advised to utilize fluoride-based toothpaste daily. Oral care is fundamental to prevent dental caries that is still amongst one of the major public health issues (Kanduti et al. 2016). 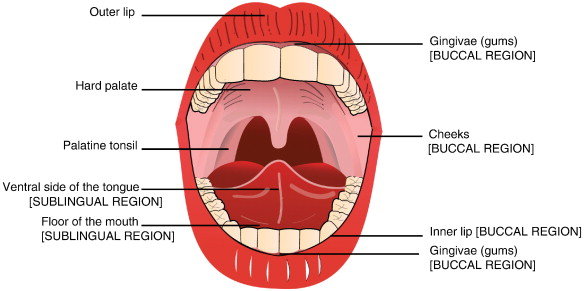 Figure 7: The anatomy of the oral cavity. (Kraan et al. 2014). The sensory pathway of taste The perception of taste is facilitated with the brain where the smell of the food is sent to the olfactory cortex. The texture and the feeling when touching also contribute to the taste (Kraan et al. 2014). The hydrophilic molecules in the food dissolved in the saliva stimulate the gustatory cells inside the taste buds in the oral activity. This stimulates the taste receptors where the peripheral information is sent to nerve fibres in the vagus, facial and glossopharyngeal nerves that associate with the brain stem (Vincis and Fontanini, 2019). They then transmit the signals to the medulla oblongata relaying them to the thalamic, subcortical and the cerebral cortex of the brain. The cerebral cortex (grey matter), subcortical (white matter) and the basal ganglia form the cerebral hemispheres. The convergence and divergence of information are then integrated into the central nervous system with the sensory system and the homeostatic, visceral and other processes ( Vincis and Fontanini, 2019). The power of touch Temperature, vibration, pressure, pain, the texture of an object are all different tactile sensations that can be felt via various receptors on the skin and relays the signal and travels to the brain via the peripheral nerves and can influence the reaction. The skin has three fundamental layers: an outer epidermis, middle dermis and inner hypodermis as presented in Figure 8. Merkel cells are receptors found in the basal layer of the epidermis of the hands, external genitalia and the lips. Meissner corpuscles are situated in the upper dermis of the feet soles and tips of fingers where there is no hair. The Pacinian corpuscles, Merkel and Meissner corpuscles can sense the touch, vibration and pressure stimulus, for instance, pain, itch and avoiding speech. Allah (The Most High) states: "And indeed, every time I invited them that You may forgive them, they put their fingers in their ears, covered themselves with their garments, persisted, and were arrogant with [great] arrogance." [Quran, Surah Nuh, 71:7] Other features of the skin consists of: Krause end bulbs that sense coldness whereas Ruffini cylinders sense the heat (Al-Ghazal, 2006). Another example is when feeling the pain stimulus, in the earlier generations, it was thought that the whole body senses the pain stimulus. However, the transmission of the pain and heat sensation from the nerve endings of the skin to the brain was later discovered. There are two types of afferent systems that elucidate pain sensations: epicritic and protopathic (Head, 1920; Price, 2007). Epicritic pain is localised and can sense a prick of a needle, or a slight alteration of temperature (Price, 2007). On the other hand, protopathic pain has a slow onset that can constantly feel pain repeatedly (Head, 1920). However, pain cannot be felt nor processed to the brain if the nerve endings are damaged, for example, after burning your hand severely. Allah (The Most High) states in the following verse: "Those who disbelieve in Our verses, We will drive them into a fire, every time their skins are roasted We will replace their skins with other new skins so that they may taste the torture. Allah is ever Exalted in Might and Wise." [Quran, Surah Nisa, 4:56] Al-Ghazal (2006) emphasised in relation to this verse that due to the severity of the nerve endings, those who enter the Fire cannot feel pain as it is not transmitted to the brain. This is why the burnt skin is replaced with fresh skin to feel the pain sensation. This further highlights the authenticity of the Quran that highlights this physiological and scientific fact before discoveries of man. Moreover, our fingerprints are unique even with monozygotic twins and have been mentioned by Allah (The Most High) centuries ago. Scholars have mentioned that they recreated people based on the fingertips that include the DNA. Allah (The Most High) states: " Yes indeed; We can reconstruct his fingertips. On Resurrection Day, Allah will reconstruct our bodies to the smallest detail even our unique fingerprints." .[Quran, Surah, Verse 4] 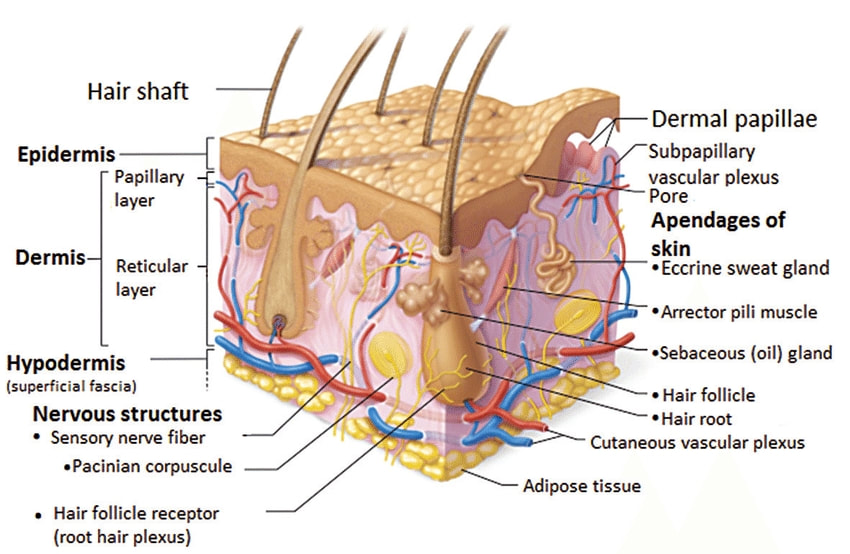 Figure 8: The structure of the skin (Lihacova, 2015) The power of proprioception Proprioception otherwise known as kinaesthesia is considered the sixth sense. It focuses on position, movement and balance of our limbs, muscles and joints and this in turn; allows people to touch (Proske and Gandevia, 2012). So why is it not considered a touch sense? Proprioception is the ability to sense muscle force, weight, effort, viscosity and movement as opposed to what it touches, for instance, texture, feeling and signals of pain. Allah (The Most High) states: “And [mention, O Muhammad], the Day when the enemies of Allah will be gathered to the Fire while they are [driven] assembled in rows. Until, when they reach it, their hearing and their eyes and their skins will testify against them of what they used to do. And they will say to their skins, "Why have you testified against us?" They will say, "We were made to speak by Allah, who has made everything speak; and He created you the first time, and to Him you are returned. And you were not covering yourselves, lest your hearing testify against you or your sight or your skins, but you assumed that Allah does not know much of what you do” [Quran, Surah Fussilat 41: 19 – 22] In our body, there are three types of muscle tissues: skeletal, cardiac and smooth muscles. The morphology of the muscle fibres differs in each type. The cardiac muscle is striated and arranged in bundles. It has an involuntary control mechanism and resides in the heart to help circulate blood around the body. There are mitochondria in the cells required for respiration. Similarly, skeletal muscles also have a striated feature and are essential for voluntary movement where it is attached to the muscle via the tendon. The skeletal muscle has repeated thin spherical long chains of the actin protein filaments and is surrounded by thick protein filaments (myosin) to create the bundling feature and; slide passed each other for the muscles to contract. The thin actin filaments have a myosin-binding site which allows the spontaneous bonding with myosin to occur. When the myosin binds, it undergoes a conformational change and; this causes the thin filament to move. The thin filaments are attached to a dense protein plate called a Z disc that anchors them. On the other hand, the smooth muscle has a striated feature and functions in protecting internal organs such as the stomach and provide involuntary muscle contractions. The sensory pathway of proprioception There are kinaesthetic receptors/mechanoreceptors to detect stretch and other movements in the effector muscles, skin, tendons and joints. The signal is transmitted to the motor input to control movement (Taylor, 2009). The afferent nerves affect the tone and postural reflexes (Aman et al. 2014). The proprioceptive sensations differ from the exteroceptors in the ear and eye (Proske and Gandavia, 2012). Thixotropy allows tension and stiffness that is exhibited by the muscle spindles and the skeletal muscles. Input from primary endings of muscle spindle aid in the position and movement; whereas secondary endings of the muscle spindles are linked to a sense of position (Tsay et al. 2015). 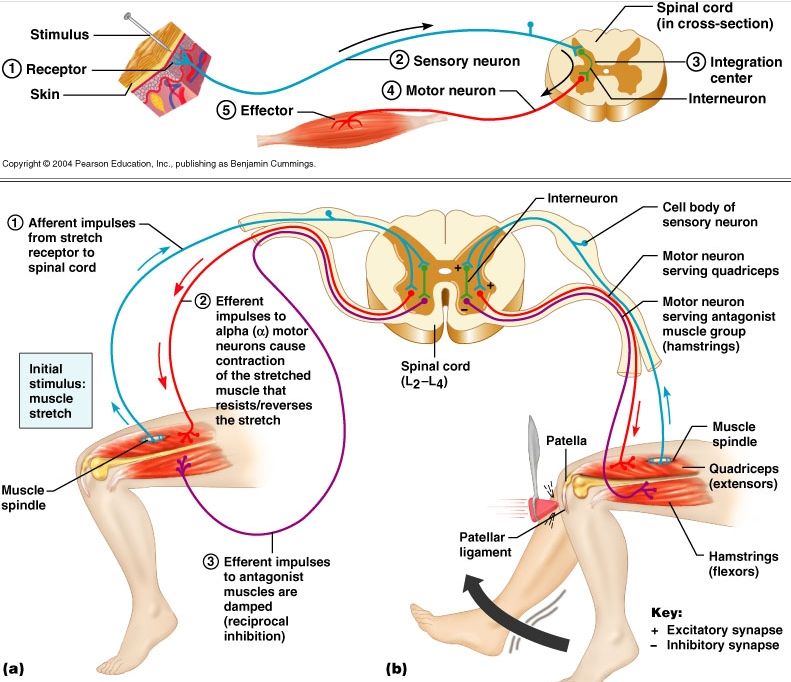 Figure 9. The sensory pathway of propriception (Cummings, 2004) Overall, we have six senses: hearing, sight, smelling, taste, touch and proprioception where they transmit the peripheral information to the brain to facilitate how we perceive the world around us. Advancement in neuroimaging, for instance, magnetic resonance imaging (MRI) assists in observing the proprioceptive stimuli and the integrative input of other senses. This has all been created by Allah (The Most High) and; we will be accountable for what we do with our senses. Our physical and spiritual senses interrelate our behaviour, emotions and thoughts. A combinatorial approach in the Quran, Sunnah, Medicine and Science teaches the knowledge, spiritual and moral doctrines to learn and understand the human senses how to use our six senses, manage it with responsibility and provide benefits to humanity (Fathil et al. 2015). Next month, I aim to go more in-depth with the anatomy and physiology of the brain and what evidence in the Quran and Sunnah that associates with it.  References Alberti, P. (2006) The Anatomy And Physiology Of The Ear And Hearing https://www.who.int/occupational_health/publications/noise2.pdf
Allen, F. and Schwartz, M., (1940) The Effect Of Stimulation Of The Senses Of Vision, Hearing, Taste, And Smell Upon The Sensibility Of The Organs Of Vision. The Journal of General Physiology, 24(1), pp.105-121. Al-Ghazal, S. (2006) Medical Miracles of the Quran. UK: Islamic Foundation. Al-Nahlawi, A.R. (1983). The principle of Islamic education and its methods. Syria: Dar al-Fikr Alper, C., Luntz, M., Takahashi, H., Ghadiali, S., Swarts, J., Teixeira, M., Csákányi, Z., Yehudai, N., Kania, R. and Poe, D., (2017) Panel 2: Anatomy (Eustachian Tube, Middle Ear, and Mastoid—Anatomy, Physiology, Pathophysiology, and Pathogenesis). Otolaryngology–Head and Neck Surgery, 156(4_suppl), pp.S22-S40. Altundag, A. and Cayonu, M., (2016) Chemical Senses in Cancer Patients. Current Pharmaceutical Design, 22(15), pp.2264-2269. Aman, J., Elangovan, N., Yeh, I. and Konczak, J., (2015) The effectiveness of proprioceptive training for improving motor function: a systematic review. Frontiers in Human Neuroscience, 8. p1075 Bishop, B. (1980) Pain: its physiology and rationale for management. Part I. Neuroanatomical substrate of pain. Physical Therapy 60 (1) pp.13-20. Blaus, B. (2020) Anatomy of the Eye Image Available [online] http://www.digitaljournal.com/topic/Anatomy%20of%20the%20Eye Catala, M. and Kubis, N. (2013) Gross anatomy and development of the peripheral nervous system. Handbook of Clinical Neurology 115 pp. 29-41. Cauna N. (1982) Blood and nerve supply of the nasal lining. In: Proctor DF, Anderson IB, ed. The nose. Amsterdam: Elsevier Biomedical Press; p. 45–70. Chaudhary, Y (2020) Tadabbur (Reflecting upon the Qur’an Series) Available [online] https://sacredtexts.co.uk/2018/05/28/tadabbur-reflecting-upon-the-quran-2/ Cohen, B. (2013) Paediatric Dermatology 4th ed. Available online: https://www.sciencedirect.com/topics/medicine-and-dentistry/oral-cavity Connel, D.C. and Fregosi, R.F. (1993) Influence of nasal airflow and resistance on nasal dilator muscle activities during exercise. Journal of Applied Physiology 74 pp. 2529–2536. Dar al-Iftaa Al-Missriyyah (2020) What bearings do visions have in Islam?Available [online] https://www.dar-alifta.org/Foreign/ViewFatwa.aspx?ID=5839 Dion, M.C, Jafek, B.W and Tobin, C.J. (1978) The anatomy of the nose: external support. Archives of Otolaryngology 104 pp. 145–150. Dubin, A. and Patapoutian, A. (2010) Nociceptors: the sensors of the pain pathway. Journal of Clinical Investigations 120 (11) pp. 3760-72 Farjo, A.A, McDermott, M.L. and Soong, H.K. (2009) Corneal anatomy, physiology, and wound healing. In: M Yanoff, JS Duker, eds. Ophthalmology, 3rd ed. Edinburgh, Mosby Elsevier: Elsevier Inc., pp. 203– 8. Fathil, Mohd & Saam, Zulfan & Sukendi, Sukendi & Nizar, Syamsul. (2015). Islam and the Environment: Education Perspective. AL-Ta lim. 22. 96. 10.15548/jt.v22i2.128. Fulkerson, M., (2014) Rethinking the senses and their interactions: the case for sensory pluralism. Frontiers in Psychology, 5. p.1426. Gadhvi M and Waseem M. (2020) Physiology, Sensory System. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; Available from: https://www.ncbi.nlm.nih.gov/books/NBK547656/ Garrity, J. (2020) ‘The Optic Pathway’ Available online: https://www.msdmanuals.com/en-kr/professional/eye-disorders/optic-nerve-disorders/the-optic-pathway Geurkink, N., (1983) Nasal anatomy, physiology, and function. Journal of Allergy and Clinical Immunology, 72(2), pp.123-128. Ghanty, I. and Schraag, S., (2019) The quantification and monitoring of intraoperative nociception levels in thoracic surgery: a review. Journal of Thoracic Disease, 11(9), pp.4059-4071. Head, H. (1920) Studies in Neurology. London: Oxford University Press. Ibn Abidin, M. (1979) Radd Al-Mukhtar ala Durr al-Mukhtar Sharh Tanwir al-Absar Beirut: Dar al-Fikr. Ibn Qayyim Al-Jawziyah, M. (1991) Al-Wabil Al-Sayyib wa Rafi Al Kalim Al-Tayyib Cairo: Dar Al-Hadith. Ibn Qayyim Al-Jawziyah, M. (2018) Madarij Al-Salikin: Bena Manazil Iyyak Na’bood wa iyyak Nastaeen (Ranks of The Divine Seekers). Dar Al Hadith Ibn Sina (1952) Avicenna's Psychology: An English Translation Of Kitab Al-Najat, Book 2, Chapter 6; With Historico-Philosophical Notes And Textual Improvements On The Cairo Editon London: Oxford University Press. InformedHealth.org (2016) How does our sense of taste work? Institute for Quality and Efficiency in Health Care (IQWiG). Irvine, K. and Clark, J., (2017) Chronic Pain After Traumatic Brain Injury: Pathophysiology and Pain Mechanisms. Pain Medicine, 19(7), pp.1315-1333. Jones, N., (2001) The nose and paranasal sinuses physiology and anatomy. Advanced Drug Delivery Reviews, 51(1-3), pp.5-19. Kanduti, D., Sterbenk, P. And Artnik, B (2016) Flouride: A Review of use and effects on health. Mater Sociomedicine. 28 (2) p. 133-137. Knight, J., Wigham, C. and Nigam, Y. (2017) Anatomy and physiology of ageing 6: the eyes and ears. Nursing Times [online]; 113: 7, 39-42. Kraan, H., Vrieling, H., Czerkinsky, C., Jiskoot, W., Kersten, G. and Amorij, J., (2014) Buccal and sublingual vaccine delivery. Journal of Controlled Release, 190, pp.580-592. Lihacova, Ilze. (2015). Evaluation Of Skin Oncologic Pathologies By Multispectral Imaging Methods. 10.13140/RG.2.2.12585.70242. Masland, R.H. (1986) The functional architecture of the retina. Scientific American; 255 pp.102– 11. McWilliams, M. (2008) Foods: experimental perspectives. 6th ed. Ohio: Pearson Prentice Hall p. 45-52. Muhamad, A., Syihab, A.H. and Ibrahim, A.H. (2020) Preserving Human–Nature’s Interaction for Sustainability: Quran and Sunnah Perspective. Science Engineering Ethics 26, pp. 1053–1066. Müller, L.J, Marfurt, C.F, Kruse, F., Tervo, T.M.T. (2003) Corneal nerves: structure, contents and function. Experimental Eye Research; 76 pp. 521– 42. Omar, A. And Ibn Hanbal, A. (2004) Imam Ahmad Bin Muhammad Bin Hanbal: USA: Noor Foundation. Price D. (2007) First and Second Pain Assessment (First Pain, Pricking Pain, Pin-Prick Pain, Second Pain, Burning Pain). In: Schmidt R., Willis W. (eds) Encyclopedia of Pain. Springer, Berlin, Heidelberg. Proctor, D.F. and Adams, GK III. (1976) Physiology and pharmacology of nasal function and mucus secretion. Pharmacological Therapy. 2 pp. 493–509. Proske, U. and Gandevia, S., (2012) The Proprioceptive Senses: Their Roles in Signaling Body Shape, Body Position and Movement, and Muscle Force. Physiological Reviews, 92(4), pp.1651-1697. Ranson, S.W. and Clark, S.L (1959) Anatomy of the Nervous System. Philadelphia: WB Saunders Co. Rehwaldt, M, Wickman, R, Purl, S, Tariman, J, Blendowski, C., Shott, S., Lappe, M. (2009). Self-care strategies to cope with taste changes after chemotherapy. Oncology Nursing Forum. 36(2): E47-E56. Richardson, J., Holmes, E. And Mueller, W., (1939) Anatomy And Physiology Of The Ear. Archives of Otolaryngology - Head and Neck Surgery, 29(3), pp.560-577. Sabale, A., Kulkarni, A. and Sabale. (2020). Nasal In Situ Gel: Novel Approach for Nasal Drug Delivery. Journal of Drug Delivery and Therapeutics. 10. 183-197. 10.22270/jddt.v10i2-s.4029. Sahin-Yilmaz, A. and Naclerio, R., (2011) Anatomy and Physiology of the Upper Airway. Proceedings of the American Thoracic Society, 8(1), pp.31-39. Sawaluddin, S., Hitami, M., Darussamin, Z. and Sainab, S., (2018) The Potential of the Senses in Al-Quran as the Basic Elements of the Human Physic and Its Application in Learning. Proceedings of the International Conference on Islamic Education (ICIE 2018). Schiffman, SS. (2007) Critical illness and changes in sensory perception. Proceedings of the Nutrition Society. 66: 331-345. Schubert, H.D. (2009) Structure and function of the neural retina. Marmor MF. Retinal pigment epithelium. Roh S, Weiter JJ. Retinal and choroidal circulation. In: M Yanoff, JS Duker, eds. Ophthalmology, 3rd ed. Edinburgh, Mosby Elsevier: Elsevier Inc., pp. 511– 21. Sempo, M., Salam, R., Mohd, R., Zainudin, W., Zainol, Z., Zaki, Z., Ibrahim, M. and Sayuti, M., (2017) The Quranic Philosophy on Superiority of Audio Sense Against Visual Sense Based on the Book of Exegesis and Science Reports. Advanced Science Letters, 23(5), pp.4765-4768. Shannan, B. (2010) Audiology - A Curriculum for Excellence Available [online] http://www.ssc.education.ed.ac.uk/courses/deaf/dnov10i.html Sokolowski, B., (2007) Sensory Systems. xPharm: The Comprehensive Pharmacology Reference, pp.1-5. Taylor, J., (2009) Proprioception. Encyclopedia of Neuroscience, pp.1143-1149. Thanc Foundation (2020) Nose & Sinus Cancer Anatomy Available [online] https://thancguide.org/cancer-types/nose-sinus/anatomy/ Tsay, A., Giummarra, M., Allen, T. and Proske, U., (2016) The sensory origins of human position sense. The Journal of Physiology, 594(4), pp.1037-1049. van Stralen, H. E., and Dijkerman, H. C. (2011). Central touch disorders. Scholarpedia 6(10), 8243. Vincis, R. and Fontanini, A., (2019) Central taste anatomy and physiology. Handbook of Clinical Neurology, pp.187-204. Willoughby, C., Ponzin, D., Ferrari, S., Lobo, A., Landau, K. and Omidi, Y., (2010) Anatomy and physiology of the human eye: effects of mucopolysaccharidoses disease on structure and function - a review. Clinical & Experimental Ophthalmology, 38, pp.2-11. Zhu, J., Zhang, E. and Rio‐Tsonis, K., (2012) Eye Anatomy. eLS,.
0 Comments
Leave a Reply. |
Archives
February 2021
Categories
All
|
 RSS Feed
RSS Feed