the EXTRAORDINARY tubular network of the small intestines and conclusion of the research project2/5/2021 The small intestine is the longest organ in the human body. It is the major site where food is broken down (digested) and the small soluble molecules, electrolytes and water are then absorbed into the systemic blood circulation with a minimal diffusion rate. The presence of microscopic projections called villi and microvilli in the intestinal wall increases the surface area of absorption for molecules to be transported to tissues and glands via the blood (OpenStax, 2021). Therefore, the small intestine is adapted for digestion and absorption because of the presence of enzymes, the regulation of gut hormones, motility, villi, and immunological factors for the microbiota homeostasis to ensure no harmful microorganisms such as bacteria enter the human body system (Campbell, 2016; Collins et al., 2020; Walters 2003). Besides, waste gases, for instance, carbon dioxide are removed and exhaled (Collins et al., 2020). Last month, we discussed the link between the anatomy and physiology of the musculoskeletal system with the Quran and Hadith. We also discussed how the bone and intestines are associated, particularly the microbiota. One of the molecules absorbed is the calcium ions and the malfunction of the bone has been found in lactose intolerance, coeliac disease, short bowel syndrome, bacterial overgrowth, and Crohn’s disease (Campbell, 2016; Augustyn et al., 2019). Therefore, understanding how the small intestine functions creates a framework of identifying pathways to treat gastrointestinal diseases (Volk et al. 2017; Zheng et al. 2020). Allah (The Most High) has revealed how the organs were nourished by the gastrointestinal system in the following verse: “Verily, in cattle there is a lesson for you. I give you drink from their insides, coming from a conjunction between the digested contents (of the intestines) and the blood, milk pure and pleasant for those who drink it.” [Quran, Surah Al Nahl (The Bee) 16:66] This highlights the role of enzymes in digesting food is primarily found in the mouth, stomach, pancreas, and small intestine. Ibn Kathir (2000) mentioned concerning this verse, that it is about one cattle or a herd of cattle, for we can provide a drink from their bellies. Also, the blood and milk have a defined route when the food is digested in the stomach i.e., the blood goes to the veins whereas the milk goes to the udder, the urine is excreted via the bladder and the faeces is excreted via the anus. The design of how Allah (The Most High) created the cattle is mirrored with what occurs in the human body where each defined route is not affected by the other. Subhanallah! For example, the difference in the pulmonary and systemic circulation in the human body where the former is involved with the lungs and the latter is involved to provide for body tissues. “So, which of the favors of your Lord would you deny?” [Quran, Surah Al Rahman (The Most Gracious) 55:13] The development of the small bowel in the foetus occurs in week 3; this is where gastrulation occurs. Gastrulation is where the tubular network and glands are formed in the primitive gut and consist of three germ layers: endoderm, mesoderm, and ectoderm (Moore, 1986). The process is regulated by the Hox signalling pathway primarily by the following genes: SOX9; FOXA2 and GATA4 (Volk et al., 2017). The midgut begins to open and associate with the disc of the embryo ca. week 4 (Fish and Burns, 2020; Moore, 1986). The lumen of the small intestine and the yolk sac form the vitelline duct. The development of the gut progresses over the weeks, the loop herniates on the umbilicus and this increases the surface area of the small intestine, large intestine, liver and kidneys to develop further (Collin et al., 2020). The epithelium undergoes various turnovers via stem cells. The endodermal layer forms the inner epithelial lining; the splanchnic mesoderm forms the muscular connective tissue, the jejunum and ileum derive from the midgut and the foregut from the duodenum (Collins et al., 2020). The cuboidal cells set up the basis for the villi to form (Collins et al., 2020). At week 10 of gestation, the small intestine moves to the abdomen and by week 11 the process is completed, and the crypt, villi and microvilli are produced (Fish and Burns, 2020). The neural crest cells produce the enteric nervous system by week 13 of gestation and the vagal nerve is the main nerve involved in the small intestine (Volk et al., 2017; Moore, 1986). Anatomy and Physiology of the small intestine.The small intestine is an important organ of the digestive system. This is where most of the food is digested, and nutrients are absorbed to allow the body tissues to undergo cellular and biochemical processes at a peak level. It is linked to the large intestine as presented in Figure 1 where the water and electrolytes are absorbed (Volk et al., 2017). The approximate length of the small bowel is 3 to 5 metres. It is divided into three sections: duodenum, jejunum, and ileum (Collins et al. 2020). This is ca. five times longer than the large intestine but smaller in diameter (Nigam et al., 2019). Volk et al. estimated the length of the small intestine is ca. 6 metres (Volk et al. 2017). This indicates that the mass and length of the small intestine takes a great portion of the abdominal cavity. The duodenum is the first and shortest section of the small bowel and is approximately 20 - 25 cm (Nigam et al., 2019). It is C-shaped where the proximal end of the duodenum is linked to the antrum of the stomach (pyloric sphincter) whereas the distal end is the start of the jejunum in the peritoneal cavity. The duodenum is further subdivided into superior, descending, horizontal and ascending duodenum (OpenStax, 2020). The superior sub-section is peritoneal, and the remainder of the duodenum is retroperitoneal (Collins et al., 2020). The chyme (partially digested food) that enters the duodenum is under acidic conditions due to the presence of hydrochloric acid in the stomach. It is mixed with enzymes from the pancreas, the bile from the liver, bicarbonate ions secreted by the duodenum, Brunner’s glands in the submucosa secretes an alkaline-based mucus that acts as a protective barrier against the acidic conditions (OpenStax, 2020; Collins et al., 2020). The presence of the ligament of Treitz comprises of skeletal muscle tissue that binds the duodenal-jejunal flexure. The bile duct and pancreatic duct join at the hepatopancreatic ampulla situated in the duodenal wall where it enters the duodenum through a tiny structure called the major duodenal papilla. The amount of bile and enzymes that enter the duodenum is regulated by the hepatopancreatic sphincter (sphincter of Oddi) (OpenStax, 2020).  Figure 1: The digestive system The jejunum initiates at the duodenojejunal flexure and ends at the ileal section. It is distinctively different from the other sections of the small bowel due to the absence of Brunner's glands and Peyer's patches present in the duodenum and ileum, respectively. Its length is ca. 2.5 metres (Nigam et al., 2019). Other sources suggest the length is ca. 0.9 m (OpenStax, 2020). The primary function of the jejunum is the absorption of nutrients into the blood. Amongst the nutrients are glucose, fatty acids, glycerol, and amino acids. The jejunum is adapted for the absorptive function due to the presence of muscular flaps (plicae circulares), circular folds (Kercking valves), villi and microvilli. The Kercking valves are present near the mucosa and they flow in a spiral manner to increase the absorption rate. Microvilli are smaller finger-like projections than villi with an approximate length 1μm (0.001mm) and are present in the mucosal epithelial cells. They increase the surface area for absorption ca. 20-fold than villi (Fish and Burns, 2020). Villi are 0.5 – 1mm in length and have a capillary network comprising of an arteriole and venule where the latter allows glucose and amino acids to be absorbed directly into the blood whereas the fatty acids and glycerol are absorbed into the lymphatic vessels via the lacteals (Fish and Burns, 2020). The ileum is the longest section of the small intestine and is ca. 3 metres where it connects to the caecum of the large intestine via the ileocecal sphincter/valve as presented in Figure 2 (Collins et al., 2020). Other sources it is ca. 1.8 m in length and has a thicker vascular tissue with further mucosal folds (OpenStax, 2020). The function of the ileum is to absorb vitamin B12 and bile who were not absorbed in the duodenum nor jejunum - to be recycled (Collins et al., 2020). Another function of the ileum is to prevent the reflux of bacteria from the large intestine. The distal ileum has Peyer’s patches in the mucosa, a lymphoid tissue (lymphoid follicles) to prevent the bacteria from entering the blood (Fish and Burns, 2020). The number of Peyer's patches decreases with age (Fish and Burns, 2020). Besides, the dendritic cells in the mucosa sample the antigen from the blood, food, and microbiota. This modulates the activity of lymphocytes (CD8+ and CD4+) (Pederson et al., 2019). The ileal section is under hormonal and nerve control.  Figure 2: The intestinal lining the layers of the small intestineThere are several layers in the small intestine: the inner layer is lined by mucosa responsible for the maximal absorption where enterocytes have the villi and crypt. The crypt cells are involved in proliferation and convert to enterocytes, Paneth cells, goblet cells and enteroendocrine cells (K and S) (Collin et al. 2020). The goblet cells secrete mucus in the intestinal glands and epithelium (OpenStax, 2020). Paneth cells secrete lysozymes that conduct a bactericidal action for macrophages to engulf them via phagocytosis (OpenStax, 2020). The MK and K cells secrete the insulinotropic peptide; a regulatory hormone that releases insulin. The S cells secrete secretin (OpenStax, 2020). Other cells found in the intestinal glands are G and I cell that secretes gastrin and cholecystokinin respectively. Cholecystokinin releases the pancreatic enzymes and bile. The M cells secrete motilin whose function is to increase the emptying of the stomach via peristaltic movement. It also stimulates the production of pepsin. The M cells are situated in the intestinal glands of duodenum and jejunum (OpenStax, 2020). The outermost layer is the serosa where it is subdivided into mesothelium and epithelium. These cells have a short life span of 3 to 5 days and therefore, has a high renewal rate (Collins et al., 2020). The middle layers of the small intestine are the muscularis and submucosa. The muscularis consists of smooth muscle, the outermost layer contains longitudinal muscle that shortens and elongates whereas; the innermost layer is a circular muscle that causes constriction. The presence of nerves between both muscle types increases the motility of the food from the proximal end to the distal end to conduct the chemical digestion (Collins et al. 2020). The submucosa is a connective tissue comprising of nerve, blood, and lymph supply (Collins et al., 2020; Hundt et al., 2020; Stallard et al., 1994). The nerve supply of the intestines arises from the autonomic nervous system. The vagus nerve of the parasympathetic system controls secretions and motility (OpenStax, 2020). The thoracic splanchnic nerve ganglion cells are part of the sympathetic system and surround the superior mesenteric artery (OpenStax, 2020). Pain stimulus is felt at this site. The main blood supply is via the superior mesenteric artery and vein. The arterial blood initiates from the celiac trunk to the superior mesenteric artery. The venous supply joins the splenic vein to form the hepatic portal vein and the blood containing the nutrients are transporter to the liver (Collin et al., 2020; OpenStax, 2020). The lymph supply via the nodes initiates from the mucosa to the mesentery to the arterial near the superior mesentery. The lymph then flows into cisterna chyli and then thoracic ducts and joins with the jugular and subclavian vein. It is the main pathway in how fat and immune cells are transported and how tumour cells can proliferate to other organs. This may explain why there is an enlarged node known as Virchow’s node that is clinically presented in small bowel tumours (Collin et al., 2020) An insight into the digestive and absorptive mechanisms of carbohydrateS Most of the chemical digestion takes place in the duodenum; this sub-section will briefly introduce how carbohydrates are digested. Carbohydrates are large polysaccharides - long chains of sugar units called monosaccharides joined together by glycosidic bonds; for instance, starch and glycogen. It is estimated that carbohydrates account to ca. 40-45% of our calorie intake and plant starches account for 50-60% of the diet (Goodman, 2010). Some of the food we eat contain disaccharides, for instance, maltose, lactose, and sucrose. Starch consists of two types of glucose polymers: a straight chain of glucose units linked together by alpha 1-4 glycosidic bonds called amylose and a branched form of glucose units linked together by alpha 1-6 called amylopectin. It functions as storage in plants. Following mechanical digestion by the teeth, the salivary glands secret an enzyme called alpha-amylase; it forms part of the saliva present the mouth. Enzymes have high specificity whereby a specific substrate binds to its active site just like a lock and key. The substrate that binds to amylase is starch - the product formed is maltose. Maltose is a disaccharide which consists of two glucose monomers connected through an alpha 1-4 glycosidic bond. It passes through the oesophagus (food pipe) to the stomach where chyme is produced. As the chyme enters the duodenum, the pancreas releases beta-amylase that chemically digest (hydrolyses) the disaccharides to produce the glucose molecules. Additional enzymes can be found in the brush border of the small intestine. Amongst them are sucrase, maltase, trehalase, isomaltase and beta-galactosidase. For instance, maltose can be hydrolysed by maltase through the alpha 1-4 glycosidic linkages. The product is glucose that is absorbed into the blood via the villi and is also transported by carrier-mediated transporters in the apical membrane (Fish and Burns, 2020). The two main transporters involved in transport are the facilitated diffusion transporter GLUT5 and Na+-coupled secondary active transport symporter (SGLT1). GLUT5 transports fructose and SGLT1 transports galactose and glucose. Glucose can also be carried by sodium ions (Goodman; 2010; Fish and Burns, 2020). An insight into the digestive and absorptive mechanisms of proteinS Proteins primarily function in growth and repair and the total daily protein is ca. 70 - 100 g of dietary protein (Goodman, 2010). They are long chains of amino acids linked together by peptide bonds. Proteolytic enzymes are required to hydrolyse the dietary protein into amino acids and smaller peptides. Some enzymes, for instance, endopeptidase breaks the internal bonds of polypeptides whereas, exopeptidases delete one amino acid at a time from the carboxyl group and the amino terminus of the protein. The chemical digestion of proteins initiates in the stomach where the active endopeptidase, pepsin, is secreted by chief cells in the gastric mucosa. It is activated from the zymogen pepsinogen and begins to digest proteins to produce the smaller polypeptides. Approximately, ca. 10 - 15% of proteins are digested in the stomach (Goodman, 2010). Pepsin differs from other enzymes because, despite its protein nature, it functions under acidic conditions because of the hydrochloric acid. Hydrochloric acid not only kills bacteria and other microorganisms but facilitates digestion by denaturing the proteins causing unfolding (Fish and Burns, 2020; Goodman, 2010). As the chyme enters the duodenum, the pancreas releases protease enzyme (under the control of cholecystokinin) and bicarbonate through the hepatopancreatic sphincter. Bicarbonate neutralises the hydrochloric acid that increases the pH to the optimum to elevate enzyme activity. Additional enzymes are secreted in the intestines: endopeptidases (elastase, trypsin, chymotrypsin) and carboxypeptidases A and B to further hydrolyse the polypeptides to 30% free amino acids and 70% of oligopeptides (Goodman, 2010). Oligopeptides consist of 2 - 8 amino acids and are further cleaved at its amino terminus by exopeptidases to produce dipeptides, tripeptides, and free amino acids. Elastase cleaves elastin and cleaves peptide bonds adjacent to alanine, serine, and glycine. Trypsin is activated from its zymogen trypsinogen by the jejunal brush border enteropeptidase/enterokinase. Trypsin also cleaves peptide bonds of other zymogens near the arginine or lysine amino acid residues to become active enzymes. On the other hand, chymotrypsin hydrolyses peptide bonds adjacent to hydrophobic amino acids - less specific (Goodman, 2010). Carboxypeptidases cleaves the carboxyl terminus of the polypeptides and have two types that specifically releases amino acids. Carboxypeptidase A releases alanine, leucine, valine, and isoleucine whereas, carboxypeptidase B releases lysine and arginine residues. The uptake of amino acids, tripeptides and dipeptides across the enterocytes requires carrier-mediated active and facilitated transport proteins as presented in Figure 3. The type of transporter is dependent on several factors: the type of amino acid and mechanism used for transport. There are various types: amino acids: anionic (acidic), neutral, cationic (basic), and zwitterion (Goodman, 2010) If the amino acid transporter has stereospecificity, they transport peptides with L-amino acids that have a greater affinity to bind than D-amino acids. They are actively co-transported with sodium ions via the capillaries of the villi to the liver via the hepatic portal vein (Goodman, 2010). Neutral L-amino acids are absorbed across epithelial cells by entering via the secondary active Na+-dependent cotransporter and leaving with the Na+-independent facilitated diffusion transporter. Other amino acids have a broad specificity whereby some undergo active transport whereas other transport via facilitated diffusion and can bind to different types of transporters across the basolateral membrane into the blood. Oligopeptides, most dipeptides, and tripeptides are predominantly transported by PEPT1 intestinal oligopeptide transporter residing in the duodenum and jejunum. PEPT1 has a low affinity and requires a hydrogen ion electrochemical gradient that initiates from the lumen of the small bowel to the cytosol of enterocytes. This is maintained by the Na+/H+ exchange in the brush border membrane removing the sodium ions by Na+, K+-ATPases across the basolateral membrane. This explains the difference in pH between the intracellular pH of the enterocyte 7.0 – 7.2 and the pH of the brush border 6.0. The deficiency of transporters or loss of function in kidneys can cause amino acids in the urine (Goodman, 2010).  Figure 3: The absorption of peptides An insight into the digestive and absorptive mechanisms of fatS The products of the chemical digestion of lipids are fatty acids and glycerol. Lipids are initially digested in the stomach where gastric lipase cleaves 15-20% of fats and is completed by the pancreatic lipase in the duodenum (Goodman, 2010). Gastric lipase is secreted by the gastric chief cells in the fundic mucosa in the stomach. It has a pH of 3 - 6 and hydrolyses the ester bond to produce diglyceride and fatty acids. Cholecystokinin stimulates the emptying of the stomach that gives time for the lipases to digest the fats. The gallbladder is contracted to cause the hepatopancreatic sphincter to relax. The bile and pancreatic lipase are then released through the sphincter. Additional pancreatic lipases are colipase, cholesterol ester hydrolase and phospholipase A2. The bile salts can inactivate the lipase and the pancreatic colipase counteracts this. Colipase is activated by trypsin in the jejunum and binds to triglyceride (fat) that facilitates the binding between lipase and triglyceride. The bile salts emulsify fats from large droplets to small droplets and the reduction in the surface area of the fats facilitates the pancreatic lipase. The droplets convert into several forms by the addition of bile salts before producing the products: free fatty acids and 2-monoglyceride. At first, multilamellar liquid crystals are formed and are converted into unilamellar vesicles then mixed micelles (cholesterol, monoglycerides, bile salts, fatty acids, lysophospholipids) and then the final product (Fish and Burns, 2020; OpenStax, 2020; Goodman, 2010). Fatty acids are transported across the endoplasmic reticular brush-border membranes of the enterocytes and are absorbed into the blood. They are coated with lipoproteins to form chylomicrons that are taken via the central lateral of the villi to the lymph then the thoracic duct and the blood. An example of a chylomicron is the apoprotein B48 - a large, hydrophobic protein and like other chylomicrons, it is dependent on the microsomal triglycerides transport protein (MTP) binds with a dense particle to form a complex and catalyses the transfer from a triglyceride to the droplet (Goodman, 2010). A pre-chylomicron is formed between the Apoprotein B48-dense particle complex and the apoprotein AIV from the smooth endoplasmic reticulum. It is then transported to the Golgi apparatus via a specific transport vesicle to complete the process. Chylomicrons are transferred by another vesicle to the basolateral membrane to be exocytosed into the lacteal lymph vessel (Lowe, 2002; Goodman, 2010). Mixed micelles depend on the electrochemical gradient where the Na+/H+ exchange cause the water-soluble (hydrophilic) fatty acids to protonate and release. They are then bound to serum albumin and absorbed directly into the portal blood. Moreover, fatty acid translocase (FAT/CD36) mainly expressed in the proximal intestinal mucosa uptakes long chains of fatty acids into the enterocytes (Lowe, 2002). Carboxyl ester hydrolase cleaves dietary cholesterol. The uptake of cholesterol is conducted by Neimann-Pick C1-like 1 (NPC1L1). Efflux transport is conducted by ATP-binding cassette proteins (ABCG5 and ABCG8) (Lowe, 2002). Malabsorption of fats can influence the structure and function of the whole mucosa. This can lead to oily stools (steatorrhea) that are clinically presented in patients with pancreatic insufficiency and coeliac disease and may also affect the absorption of vitamin K, E, D and A. For instance, Vitamin D requires chylomicrons to be absorbed, other examples are diarrhoea and milk intolerance (Burns and Fish, 2020; Nikaki and Gupte, 2017). An insight into the digestive and absorptive mechanisms of vitamins and minerals. The vitamins vary where they are absorbed, vitamin K, A and D are lipid-soluble (lipophilic) and are absorbed passively. Vitamin B, however, is a water-soluble protein and is required for erythropoiesis, hair, nails and the contraction of muscles and conduction of nerve impulses to maintain the activity of the heart and brain. Vitamin B9 (folate) is absorbed in duodenum and jejunum (Fish and Burns 2020). Vitamin B12 binds to R protein in acid milieus of the stomach and then dissociates from the complex when reaching the duodenum. B12 (cobalamin) binds to the intrinsic factor secreted by gastric parietal cells before being absorbed into the terminal ileum and enter the enterocyte via ileal membrane receptors. It is required for the synthesis of DNA, red blood cells, metabolic process, and nerves. They are then absorbed into the blood by associating with transcobalamin II (Nigam et al., 2019). A B12 deficiency can destroy the parietal cells by autoantibodies which influences and decreases the production of hydrochloric acid. This leads to pernicious anaemia and even dementia if untreated (Nigam et al. 2019). The movement towards the large intestineFollowing absorption, the small bowel becomes less distended, and the gastroileal reflex stimulates peristalsis to move the remaining unabsorbed contents from the ileum to the caecum of the large intestine. With each motility action, the ileocaecal valve relaxes. This ensures that the meal eaten is completely emptied from the stomach and small bowel before the next meal. It takes ca. five hours for contents to leave the small intestine (Nigam et al., 2019; Hundt et al., 2020). Allah (The Most High) states regarding the large intestine: "Is the description of Paradise, which the righteous are promised, wherein are rivers of water unaltered, rivers of milk the taste of which never changes, rivers of wine delicious to those who drink, and rivers of purified honey, in which they will have from all [kinds of] fruits and forgiveness from their Lord, like [that of] those who abide eternally in the Fire and are given to drink scalding water that will sever their intestines?" [Quran, Surah Muhammad, 47:15] This complements the findings by researchers whereby boiling water can affect the peritoneum and the outer layer of the intestine where there are Pacini bodies containing nerve endings and will feel the pain. The intestines have no receptors to sense the stimulus (Al Ghazal, 2006). The large intestine absorbs water containing mineral ions and nutrients released by the bacteria and is used for metabolic processes. This solidifies the condensed faeces and is stored in the sigmoid colon and rectum where it is excreted via the anus in a process called defecation.  The evidence of hadith on the intestinesThere are several hadiths in which our Beloved Prophet (peace be upon him) refers to the intestines. One of which is the following: It was narrated by Abu Hurairah (may Allah have mercy upon him) that the Prophet Muhammad (peace be upon him) said: "A man used to eat much, but when he embraced Islam, he started eating less. That was mentioned to the Prophet who then said, "A believer eats in one intestine (is satisfied with a little food) and a Kafir eats in seven intestines (eats much)." [Al-Bukhari, Book 65, Hadith 308;309] One of the respected scholars, Al Nawawi reported that the most agreed opinion is some believers eat one intestine and most non-believers eat seven intestines. It does not necessitate that each one of the seven intestines is like that of the believer. The hadith emphasizes that one needs to be content with little from this temporary world and eating a lot can have a negative effect and the opposite. This also links with the following verse from the Quran where Allah (The Most High) states: “O children of Adam, take your adornment at every Masjid, and eat and drink, but be not excessive. Indeed, He likes not those who commit excess.” [Quran, Surah Al-Araf (The Heights); 7:31] Regarding this verse, Al Sarakhsi mentioned in his book Al-Mabsoot: "That is because one eats to benefit himself; so, there is no benefit in eating more than one's fill for it causes harm. Accordingly, this will be like throwing food in garbage or worse than that. Also, other people have a right in the food that is more than one's need for it may stratify another person's hunger if it reaches him with or without a return. Thus, eating it involves a violation of the right of others and this is something prohibited. Moreover, eating more than one's fill may cause diseases and thus this will be a form of hurting oneself." Therefore, it is important to maintain a balanced diet where Prophet (peace be upon him) said: "The son of Adam cannot fill a vessel worse than his stomach, as it is enough for him to take a few bites to straighten his back. If he cannot do it, then he may fill it with a third of his food, a third of his drink, and a third of his breath." [Al-Nasai 4:178, Al-Tirmidhi, Ahmad 4:132; Tuhfat Al Ahwadhi 7:51] Tumours of the small intestineSmall intestinal cancers are rare and around 1,700 people are diagnosed annually between the period 2015 - 2017 where ca. 790 in females in 2017 and ca. 970 in males in 2017 (Cancer Research UK, 2021). It is prevalent amongst people aged 80 to 84. The use of techniques, such as molecular profiling and enteroscopy allows tumours to be diagnosed early leading to therapeutic modalities. However, the survival rate remains the same and this is because of the lag time. However, the use of cancer waiting times allowed tumours to be diagnosed most quickly - progress (Islam et al., 2014; Pedersen et al., 2019). The main type of small intestinal cancer is the small bowel adenocarcinoma (Pedersen et al., 2019). This research area has increased because many previous studies observed how colorectal cancer (tumours of the large bowel) can metastases to this defined region which allows it to be resectable. The cause of this rare tumour is due to several respects: firstly, the dilute food contents have fewer effects on the duodenal mucosa than the large intestine. There is also a difference in the redox microenvironment where there are less reactive oxygen species (ROS) in the small intestine than the large intestine. Therefore, DNA adducts are readily formed in the large intestine and this causes DNA damage, and this influences the immunological control than the small intestine. This occurs despite dendritic cells are present in the mucosa and the release of interleukin 10 against the cell transformation. The levels of ROS can increase due to several risk factors: smoking cigarettes and alcohol (Pedersen et al., 2019). The role of microbiota homeostasis in promoting or suppressing tumorigenesis and proliferation in the small intestines is still ongoing (Pedersen et al. 2019). Patients with commodity conditions i.e., coeliac disease and Crohn's disease are also at risk. Other causes of small bowel cancer could be genetically linked where germline mutations in genes involved in DNA mismatch repair MLH1, MSH2, MSH6, PMS2 have been revealed and may also affect colorectal cancers that require immune checkpoint therapy. Moreover, patients with familial adenomatous polyposis that occurs in the early the onset of colorectal tumours have a 4.5% chance of developing small bowel adenocarcinoma (Pedersen et al., 2019). The clinical presentation of small bowel adenocarcinoma is normally intermittent abdominal pain. Other symptoms include nausea, weight loss and gastrointestinal bleeding, however, the latter can be misinterpreted as iron deficiency anaemia because of the negative outcome of the colonoscopy test (Pedersen et al., 2019). The rarity of this cancer did not allow a screening programme to be established like the NHS large bowel screening programme. However, it can be diagnosed through radiological imaging to determine whether it has progressed from the colon. CONCLUSION OF RESEARCH PROJECTOverall, we have reached the end of my six/seven-month 40,803-word literature review (excluding references and tables) titled: 'The link between medicine and science with the Glorious Quran... with a focus on anatomy and physiology'. It was divided into six sections:
The two foundations of Islam are Quran and Hadith that teach us to respect, learn tolerance of other religions, and persuade us to be successful in medicine and science. The Greek medical and scientific writing was translated to Arabic in Syria, Egypt and Iraq. This led to Arabic become a language of not only the Quran but a language of effective diplomacy, learning and long-lasting innovations. The Quran has been written in the traditional language of Arabic. It comprises of 114 chapters and 6237 verses distributed to Prophet Muhammad (peace be upon him) over 23 years which comprised of 13 years in Makkah and 10 years in Madinah. The Quran consists of parables of the Prophet, divine nature, social justice, and lessons that we can learn and apply once a thorough understanding is gained because some verses can be misinterpreted and it is through the scholars of exegesis (Tafsir) one can thoroughly understand what is meant by what is said (Ibn Kathir, 1990). This provides feelings of peace, calmness, patience, and tranquillity. Naturally, the pandemic can cause upset but through reading the Quran one can counteract this. Allah (The Most High) states: “There is no god but He: That is the witness of Allah, His angels, and those endued with knowledge, standing firm on justice. There is no god but He, the Exalted in Power, the Wise” [Quran, Surah Al Imran (Family of Imran) 3:18]. There were several questions asked by readers and I wanted to leave it till the end. One of the lessons I learnt from Surah Kahf, is when Prophet Moses (peace be upon him) accompanied Khidr on his journey and the Prophet wanted to find out the reason why Khidr did a particular action for each event and each time, Khidr replied '“Did I not say that with me, you would never be able to have patience?”' [Quran, Surah Kahf, 73:74] First question: What made you start this project? Like everyone else, I was also affected by the coronavirus pandemic and I tried to respond to it in a positive mindset by increasing my relationship with Allah (The Most High) through the Quran more than a normal day, being surrounded by my loved ones and my zeal for learning new things. I wanted to combine my interests in medicine, research and the Quran. We can easily count the effects of the pandemic, however, the blessings we have within us and around us are countless. The engineering mechanisms of how our bodies function have been designed and created by Allah (The Most High) - no one can ever reach its status. How have we existed? How cells interact with one another? How are nutrients circulated? How is movement conducted? The visual concepts and other senses that involve emotion, contemplation and building of our inner faith? As a human and Muslim, I must be conscious of my meaning and purpose - and so do you. The anatomy and physiology of the human body are a piece of living evidence. It illustrates the intellectual honesty of our limits as human beings and what we know. I have spent months in my spare time reading, understanding, revising, and learning new knowledge through research - this is only a drop of the ocean. There is so much more to learn, so much more to write - seeking knowledge is part of my worship. This is merely an introduction between both fields of medicine and Tafseer. The respected scholars previous and current have studied each verse or surah or even understanding the hadith for years and continue to learn and develop. And despite their experience and present level of their knowledge, there are still aspects in the Quran and Hadith that are incomprehensible. “And those who strive in Our (cause), – We will certainly guide them to our Paths: For verily Allah is with those who do right” [Quran, Surah Al Ankabut (The Spider) 29:69]. Second question: Why is it published at 8 pm UK and not earlier? I thought that whilst searching for a job, I aimed to ensure that this project would not influence my work and family commitments. For instance, not publishing on time, so I thought publishing it in the evening will prevent this limitation inshaAllah (if Allah wills). Having a positive mindset can help with any trial, such as this pandemic. We have a duty of care to learn, ask questions and be better through observation, reasoning and productivity. It was narrated by Anas ibn Malik (may Allah have mercy upon him): “Seeking knowledge is an obligation upon every Muslim.” [Sunan Ibn Majah, 224] I thought I would continue with the planned time and share what I read and learnt. The first verse revealed to our Beloved Prophet (peace be upon him) on the 27th of Ramadan 611 AD is the following: “Proclaim! (or read!) in the name of thy Lord and Cherisher, Who created – Created man, out of a (mere) clot of congealed blood: Proclaim! And thy Lord is Most Bountiful, He Who taught (the use of) the pen, Taught man that which he knew not” [Quran, Surah Al Alaq (The Clot) 96: 1-5]. Being able to read and devote ourselves to the pursuit of seeking knowledge can protect our faith for Allah (The Most High) states: “And it is not for the believers to go forth [to battle] all at once. For there should separate from every division of them a group [remaining] to obtain understanding in the religion and warn their people when they return to them that they might be cautious." [Quran, Surah Al-Tawbah (Repentance) 9:122]. Third question: Why have you mentioned the Quran and not the hadith on the poster? I wanted to begin with Allah (The Most High) - words of the Almighty who created me and you. The main source of our life and what we recite in our daily prayers. Verily, without doubt, the Quran and Hadith are both important. The authentic hadith are collections of sayings by our Beloved Prophet (peace be upon him) by respected narrators where logic and reason with authenticity are combined and graded as Sahih. The overall evaluation and classification are known as the Mustalahul Hadith, this can prevent conflicts of principles and revelations (Hasan, 1994; Al Suyuti, 2017; Ismail et al., 2014; Moore, 1986). Similarly, as the understanding of the scholars in Tafseer and Hadith are increasing through various in-depth research, understanding the human body is also constantly evolving through various research methodologies and techniques to understand the cellular and biochemical mechanisms that affect the human body in normal physiological and pathophysiological consensus. Clinical research is fundamental in healthcare, where addressing medical needs is met through advancing knowledge to discover better treatment and procedures to improve patient outcomes. Ultimately, our physical growth may stop at puberty, but our mental and emotional growth has no end. Reading, listening, understanding and other communication skills are survival mechanisms that create new cumulative dimensions to learn something new every day no matter how new or how simple the information is (Syed, 2006). This is not limited to textbooks or articles but also involves collaborative interactions. I hope you enjoyed reading my literature review just like how I enjoyed the whole process and what you learn and what I learn is all part of our growth. So high [above all] is Allah, the Sovereign, the Truth. And, [O Muhammad], do not hasten with [recitation of] the Qur'an before its revelation is completed to you, and say, "My Lord, increase me in knowledge." [Quran, Surah Taha 20:114] referencesAl-Ghazal, S. (2006) Medical Miracles of the Qur'an UK: Islamic Foundation
Al Sarakhsi (1986) Al Kitab Al Mabsut Beirut: Dar Al-Kotob Al-Ilmiyah Al-Suyuti, A. (2017) Tadrib al-Rawi fi Sharh Taqrib al-Nawawi. Cairo: Dar Ibn Al-Jawzi. Augustyn, M., Grys, I. and Kukla, M., (2019) Small intestinal bacterial overgrowth and nonalcoholic fatty liver disease. Clinical and Experimental Hepatology, 5(1), pp.1-10. Campbell, J., Berry, J. and Liang, Y., (2019) Anatomy and Physiology of the Small Intestine. Shackelford's Surgery of the Alimentary Tract, 2 Volume Set, pp.817-841. Cancer Research UK (2021) Small intestine cancer statistics. Available [online] https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/small-intestine-cancer#heading-Zero Collins, J.T., Nguyen, A. and Badireddy, M. (2020) Anatomy, Abdomen and Pelvis, Small Intestine. Available [online] https://www.ncbi.nlm.nih.gov/books/NBK459366/ Fish, E.M. and Burns, B. (2020) Physiology, Small Bowel. Available [online] https://www.ncbi.nlm.nih.gov/books/NBK532263/ Goodman, B., (2010) Insights into digestion and absorption of major nutrients in humans. Advances in Physiology Education, 34(2), pp.44-53. Hasan, S. (1994) An introduction to the science of hadith. London: Al-Qur’an Society. Hundt, M., Wu, C.Y. and Young, M. (2020) Anatomy, Abdomen and Pelvis, Biliary Ducts. Available [online] https://www.statpearls.com/articlelibrary/viewarticle/32108/ Ibn Kathir, I. (1990) Tafsir Al-Qur’an al- ‘Adheem. Al-Zarqa: Maktabah Al-Manar. Ibn Kathir (2000) Tafsir Ibn Kathir. Saudi Arabia: Darussalam. Islam, R., Leighton, J. and Pasha, S., (2014) Evaluation and management of small-bowel tumors in the era of deep enteroscopy. Gastrointestinal Endoscopy, 79(5), pp.732-740. Ismail, T.M.S.T., Baru, R., Hassan, A.F., Salleh, A.Z.B. and Amin, M.F.M. (2014) The matan and sanad criticisms in evaluating the hadith. Asian Social Science; 10:152. Kiela, P. and Ghishan, F., (2016) Physiology of Intestinal Absorption and Secretion. Best Practice & Research Clinical Gastroenterology, 30(2), pp.145-159. Ma, Z. and Lee, Y., 2020. Small intestine anatomy and physiology. Clinical and Basic Neurogastroenterology and Motility, pp.101-111. Moore, K.L. (1986) A scientist's interpretation of references to embryology in the Qur’an. Journal of the Islamic Medical Association of North America 18:15-17. Nigam, Y., Knight, J. and Williams, N. (2019) Gastrointestinal tract 4: anatomy and role of the jejunum and ileum. Nursing Times [online]; 115: 9, 43-46. Nikaki, K. and Gupte, G., (2016) Assessment of intestinal malabsorption. Best Practice & Research Clinical Gastroenterology, 30(2), pp.225-235. OpenStax (2021) 23.5 The Small and Large Intestines Available [online] https://openstax.org/books/anatomy-and-physiology/pages/23-5-the-small-and-large-intestines Pedersen, K., Raghav, K. and Overman, M., (2019) Small Bowel Adenocarcinoma: Etiology, Presentation, and Molecular Alterations. Journal of the National Comprehensive Cancer Network, 17(9), pp.1135-1141. Stallard, D., Tu, R., Gould, M., Pozniak, M. and Pettersen, J., (1994) Minor vascular anatomy of the abdomen and pelvis: a CT atlas. RadioGraphics, 14(3), pp.493-513. Syed, I. (2006) ‘The pleasures of seeking knowledge’ Available [online] https://www.islamawareness.net/Knowledge/knowledge_article0003.html Volk, N. and Lacy, B., (2017) Anatomy and Physiology of the Small Bowel. Gastrointestinal Endoscopy Clinics of North America, 27(1), pp.1-13. Yusof, N., Che Mohamad, C. and Hassan, A., (2018) Anatomy of Musculoskeletal System in the Light of the Qur’an and Hadith. IIUM Medical Journal Malaysia, 17(1).
0 Comments
The anatomical and physiological context of the heart and how the red blood cells (erythrocytes) carry oxygen around the body via the blood was discussed last month. This was achieved using core evidence from the Quran, Hadith, and literature work by scholars in the fields of Islam and medicine. Today, this section of the project aims to continue bridging the gross anatomy and physiology of the human body with the foundations of Islam by discussing the structure and function of the bone; this is where red blood cells are made via the process known as erythropoiesis. Besides, we will also cover other elements of the musculoskeletal system, the joints, muscles, cartilages, tendons and the ligaments. In total, the bone has been stated in the Quran twelve times. Allah (The Most High) states: “Or are you not aware of˺ the one who passed by a city which was in ruins. He wondered, “How could Allah bring this back to life after its destruction?” So Allah caused him to die for a hundred years then brought him back to life. Allah asked, “How long have you remained ˹in this state˺?” He replied, “Perhaps a day or part of a day.” Allah said, “No! You have remained here for a hundred years! Just look at your food and drink—they have not spoiled. ˹But now˺ look at ˹the remains of˺ your donkey! And ˹so˺ We have made you into a sign for humanity. And look at the bones ˹of the donkey˺, how We bring them together then clothe them with flesh!”1 When this was made clear to him, he declared, “˹Now˺ I know that Allah is Most Capable of everything.” [Quran, Surah Baqarah (The Cow), 2:259] A number of respected scholars: Ibn Jarir, Ibn Abi Hatim, Ibn Abbad, Al-Hassan, Qatadah, Al-Suddi and Sulaiman bin Buradysh (may Allah have mercy upon them all) agreed that this Quranic verse is a reference to the story of Uzayr that took place in Jerusalem after Nebuchadnezzar destroyed it and killed its people (Abi Hatim, 3:1009; Al-Tabari 5:439; Al-Tabari 5:440; Ibn Kathir, 2000). He was resurrected by Allah (The Most High) and asked whether he was 'dead a day or part of the day'. Al-Hakim (may Allah have mercy upon him) in his book Mustadrak mentioned that Kharijah bin Zaid bin Thabit (may Allah have mercy upon him) mentioned that his father said that the Prophet (peace be upon him) used the term 'Nunshizuha' is in relation to adjustment. However, this was not recorded Sahih by Bukhari and Muslim (2:234). It was mentioned by Mujahid it was 'nunseeha' (Al Tabari 5:476). Al-Suddi (may Allah have mercy upon him) further added that Uzayr witnessed the bones of his donkey being collected and Allah (The Most High) covered the bones with flesh, nerves, veins and skin and brought life into the donkey via the nostrils (Ibn Kathir, 2000). This consolidated Uzayr's faith in the Almighty that He can do All things and is Most Knowledgeable (Ibn Kathir, 2000). It also presents Allah’s instructions to research closer into the gross anatomy of the bone on how ‘we construct them’ for clarity and belief. The functions of the musculoskeletal system are the movement with levers of muscles, support, and posture. For Muslims, particularly the bone is essential to perform our daily prayers (Salah) and the coccyx is the form in how humanity will be resurrected in the afterlife. In Figure 1, it illustrates the positions in which human prostate to the Almighty. This corresponds to the hadith narrated by Ibn Abbas (may Allah have mercy upon him): "The Prophet peace be upon him was ordered by Allah (The Most High) to prostrate on seven parts and not to tuck up the clothes or hair whilst praying. Those parts are the forehead along with the tip of the nose, both hands, both knees and the toes of both feet." [Al-Bukhari, 809] Ahmad (2010) shared evidence that praying increases the strength of bones and improves the spinal curvature. The strength of the muscles depends on pressure and muscle contraction. Inactivity causes the electric current in the bones between the two poles to decrease and weaken the bones. Similarly, this can also occur in space where the movement is weakened because there is no resistant force of gravity. This emphasises how atrophy can influence movement and bone metabolism. The daily prayer involves 17 units/rakaahs and this excludes the voluntary prayers. It is estimated it takes ca. two hours, on the other hand, it is important to state that there is no exact time to complete the prayer because it depends on the pace, Surah read and other factors (Ahmad, 2010). The divine energy that flows through the heart and body motivates to continue to the straight path.  Figure 1: The bone positions for prostration. Furthermore, there is also evidence of movement in the Quran, where Allah (The Most High) states: "And Allah has created from water every living creature. Some of them crawl on their bellies, some walk on two legs, and some walk on four. Allah creates whatever He wills. Surely Allah is Most Capable of everything." [The Quran, Surah Al-Noor (The Light), 24:45] Ibn Kathir (2000) mentioned that Allah created living things in different forms and colours. The snakes crawl on their bellies whilst humans and bird walk on two legs. Cattle, horses, lions, and camels are examples of living creatures that walk on 4 legs. The description of how living creatures can move ignites guidance, understanding and intellect for people to ponder. Nevertheless, there are also differences whereby despite; humans and birds both walk on two legs, they differ in the torso position and posture. Furthermore, Allah states in the following verse how man is a witness against himself. "Rather, man, against himself, will be a witness." [Quran, Surah Al-Qiyamah (The Resurrection), 75:14] Qatadah (may Allah have mercy upon him) mentioned in a narration 'By Allah! If you wish to see him, you would see him as someone who sees the shortcomings of the people and their sins, yet he is heedless of his own sins. It used to be said, "Verily, it is written in the Injil; `O Son of Adam, do you see the small splinters in the eye of your brother and disregard the tree stump that is in your eye, so you do not see it." (Al Tabari: 24:62; Ibn Kathir, 2000). Other functions of the musculoskeletal system are the formation of blood cells (haematopoiesis), maintenance of the homeostasis for calcium and phosphate mineral ions that aids in the production of cytokines and growth factors and the protection of vital organs such as the brain, heart, and the lungs because of the strength and rigidity of the bone (Clarke, 2008; Ralston, 2017). the development of the boneThe human skeleton accounts for 20% of the body weight. The number of bones of the human skeleton at birth is 98, which later develops into 270 bones (Scheuer and Black, 2000). The adult skeleton has 206 bones and this is because of the remodelling of the bones where the fusion between the bones takes place. This decreases the number of bones preserving their strength and rigidity. For instance, a child has five sections of the sacral vertebrae and develops into one section when transitioning into an adult (Scheuer and Black, 2000). The human skeleton is presented in Figure 2. There are two types of the human skeleton: axial and appendicular skeleton. The axial skeleton consists of the cranium (head), vertebrae and the neck (cervical and hyoid vertebrae)(Clarke, 2008). The appendicular skeleton consists of the upper and lower limbs, for instance, the pelvic girdle and the shoulders. In some literature, there is an additional type - the visceral skeleton that consists of the sternum, ribs, lower and upper jaw (Al-Najjar, 2005). However, other sources suggest that there are 213 bones, and this excludes the sesamoid bones: the appendicular skeleton has 126 bones, the axial skeleton has 74 bones and; there are 6 bones in the auditory ossicles (Clarke, 2008). Bones vary in size, structure, and markings and this makes it adaptable to its location and function in the human body. There are three types of bone markings: articulation, holes, and projections. Articulation is where bones are joined together that specifically fit. Holes are opening grooves in the bone that allow blood vessels and nerves to enter. The projection is found on the bone surface that serves a place where tendons join muscle to bone and ligaments bone to bone (OpenStaxCollege, n.d.). The bone consists of 25% of organic products (glycoproteins, proteoglycans, and collagens) and 75% of calcium salts.  Figure 2: The human skeleton 6During the fetal development which occurs between the 3rd and 8th week, Allah (The Most High) created the vertebrae (backbone) from cartilage before the muscles. The jawbone (mandible) is the first cartilage (Meckel's cartilage) that underwent transition into a bone on Day 41. The cartilage is a semi-rigid connective tissue that acts as a shock absorber. It provides support and adds a smooth surface for the articulation of the bones to grow and develop and perform gliding movements (Yusof et al., 2016). Three types of cartilage differ in the number of extracellular fibres: the hyaline cartilage has several fibres but do not have perichondrium and cannot regenerate new cartilage following injury, the fibrocartilage comprises of collagen fibres and the elastic cartilages contains elastic fibres (Young et al., 2006). Allah (The Most High) states: "Verily, We have created the human from a quintessence of clay; then We placed him as a drop in a fixed resting place. We then made the drop into a clot and that into a fetus. We then made bones and clothed the bones with flesh and from that brought forth another creation. Therefore, blessed is God, the very best of those who create." [Quran, Surah Al-Muminoon (The Believers, 23:12-14]Ibn Kathir (2000) mentioned concerning the bones that they were clothed with flesh to cover and strengthen the body. There are nerves and veins in the head, two arms and two legs. This highlights the uniqueness and vivid detail of the physical creation of man portrayed by Allah (The Most High). It also contemplates the findings of Wyganowska-Swiatkowska and Przystanska (2011) who discovered that at 32 days, the Meckel's cartilage developed and ossification is progressed at 41 days where a mandible is formed inferior to the cartilage where the muscles begin to form at 44 days. The formation of the bone is known as osteogenesis or ossification. It occurs from the neural crest, paraxial mesoderm or lateral plate that become somites and differentiate into sclerotome and dermatomyotome cells (Moore and Persaud, 1998). Further differentiation occurs where the sclerotome cells produce the connective mesenchyme that later forms the bone-forming cells called osteoblasts, fibroblasts and chondroblasts. There are two ways in how the bones are formed: intramembranous and endochondral ossification illustrated in Figure 3. Intramembranous ossification is where the mesenchymal cells transition into osteoblasts without the formation of cartilage. There is a high vasculature area of the embryonic connective tissue (primary ossification) and; the bones can be re-shaped to form lamellar bone. The limb buds later form the upper and lower limbs and comprise of; the apical ectodermal ridge (AER) and cuboidal ectoderm. Endochondral ossification is where the bone is produced via cartilage, the chondrocytes proliferate and undergo maturation to form bone (Tzelepi et al. 2009). The canonical Wnt/β-catenin pathway is fundamental in the differentiation of the osteoblasts, chondrogenesis and haemopoiesis (Clarke, 2008). The Wnt (wingless) proteins produce the dermatomyotome that expresses the muscle-specific genes e.g. MYF5 to stimulate the synthesis of skeletal muscles (Sadler and Langman, 2010). 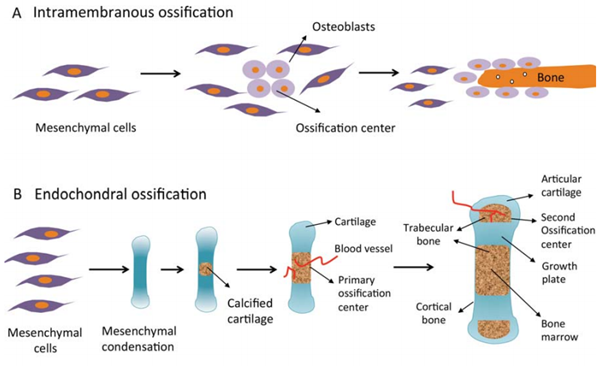 Figure 3: Ossification (Creative Biomart, 2020) the gross anatomy of the bone.The bone (osseous) tissue consists of connective tissue (collagen type I fibres) that aids in its elasticity and the mineral salts (inorganic salts) that provide its hardness and rigidity. Calcium phosphate and carbonate produce hydroxyapatite and adheres to the collagen fibres. There are additional mineral ions, for instance, fluoride, magnesium hydroxide and sulphate that calcify the collagen fibres to increase the flexibility (Clarke, 2008). The histological macrostructure of the bone is dependent on its porosity: cortical (compact) bone and trabecular bone (cancellous/spongy) bone (OpenStaxCollege, n.d.) presented in Figure 4. The human skeleton has 80% compact bone and 20% cancellous bone (Eriksen et al. 1994). There is variation in the ratio of compact and cancellous bone in the human skeleton, for instance, the femoral head has 50:50 ratio between compact to cancellous bones, respectively. On the other hand, the vertebrae have more cancellous tissue where the ratio proportion is 25:75 in respect to the ratio: compact to cancellous bones (Clarke, 2008). This highlights how the structure and the remodelling of the bone make it adaptable to its function. The microstructural unit of the bone is osteons (Haversian systems). They are 400 mm long and 200 mm wide in the compact bone (Clarke, 2008). The osteons produce concentric rings (lamellae) in the compact bone. The cancellous bone has semilunar osteons ca. 35 m thick in the lacunae producing a lattice-like matrix called trabeculae (Yusof et al., 2016). The compact bone is found in the shafts of long bones in particularly the periosteum and diaphysis. It is less metabolically active than the cancellous bone and functions in providing mechanical strength and protection from internal and external forces (Clarke, 2008). The biomechanical forces can be felt at the osteocyte syncytium of the bone via the canalicular network and the gap junctions (Clarke, 2008). Cancellous bone has rods and plates and consists of marrow cavities to bear the load. There is red marrow between the cells to provide balance and; withhold the density of the compact bone and; this lightens the weight of the bone and allow the muscles to function.  Figure 4: The anatomy of the bone TYPES OF BONESThere are four main types of bones: short, flat, long, and irregular bones. Long bones are produced by intermembranous and endochondral formation. It is found in the clavicle, humerus, ulnae, femur, radius, phalanges, and metatarsals. Short bones are found in the patella, sesamoid, carpal, and tarsal bones. Irregular bones are found in the vertebrae, coccyx, hyoid, and sacrum. Flat bones are found in the mandible, skull, sternum, ribs and scapulas and formed by membranous ossification (OpenStaxCollege, n.d.). This illustrates the unique creation of Allah (The Most High) in how he created each bone with its adaptable functions. Amongst the verses in the Quran that emphasize Allah's Divine ability to create is: “Allah is the Creator of all things, and He is the Wakil (Trustee, Disposer of all affairs, Guardian) over all things.” To him belong the maqalid of the heavens and the earth. And those who disbelieve in the Ayat of Allah such are they who will be losers. [Quran, Surah Al Zumr (The Groups, 39:62 63] This suggests that Allah (The Most High) encourages mankind to research nature and its molecular, cellular and biochemical composition to understand how they function. The Merciful even provided clues to His creation for guidance to The Truth. For Allah (The Most High) has the power to create, command and whatever He decides is fair and just (Ibn Kathir, 2000). The long bone consists of two parts: diaphysis and epiphysis. The diaphysis is a tubular shaft that initials in the proximal end of the bone and continues to the distal end. The epiphysis is the wider area of the bone. The epiphysis connects with the diaphysis at the metaphysis. The metaphysis is a narrow area that is composed of a transparent hyaline layer of cartilage and the epiphyseal plate otherwise known as the growth plate as presented in Figure 5. It then progressed to adult bones where the cartilage and epiphyseal plate transitions to osseous tissue and epiphyseal line respectively (OpenStaxCollege, n.d.). The walls of the diaphysis of the long bone are made of compact bone that is dense and hard. The yellow marrow is present in the hollow region of the diaphysis called the medullary cavity as presented in Figure 5a. There are two membranes periosteum and endosteum. There is a thin membrane that surrounds the medullary cavity called the endosteum. The red marrow fills the spongy bone of the epiphysis. There is another outer membrane that is fibrous called the periosteum that covers all the bone with exception of the connection where epiphyses form joints with other bones where there is a thin layer of articular cartilage instead of the periosteum to decrease friction. The periosteum is surrounded by thick collagen fibres called Sharpey”s fibres extending under the bone tissue. The periosteum comprises of blood and lymphatic vessels and nerves that provide a nutrient supply for the compact bones. The compact bone nourishes the spongy bone and medullary cavity that coils around the venous marrow longitudinal vein (OpenStaxCollege, n.d.). Arteries connect with diaphysis and enter through small openings called foramen. The arteries divide into ascending and descending branches that are parallel into thin-walled arterioles and capillaries (Travlos, 2006). The veins also pass-through marrow cavities and exit via foramena. The venous sinuses are thin-walled and have endothelial cells with minor basement membrane (Travlos, 2006). There are myelinated and non-myelinated nerves that have the smooth muscle of the arterioles (Travlos, 2006). The cranium has a spongy bone on each side of rhe compact bone called a dipole to protect the internal organs from fracture and injury (OpenStaxCollege, n.d.) Think about it, if Allah (The Most High) added detail to a snowflake - Figure 5b that is left for mankind to ponder and eventually melts. Contemplate on the beautiful creation of the bone presented in Figure 5a. “Which is it, of the Favours of your Lord, that ye deny?” [Quran, Surah Al-Rahman (The Most Merciful), 55:13] 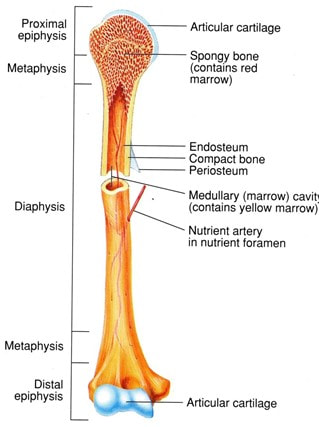  Figure 5. The creation of the bone and snowflake (a) The structure of the long bone (b) snowflake (Imster, 2019) the cellular features of the boneThere are four types of bone cells present in the osseous tissue: osteogenic cells, osteoblasts, osteocytes, and osteoclasts. The undifferentiated osteogenic cells arise from pluripotent stem cells under optimal conditions. It resides in the periosteum and bone marrow and has a high mitotic activity to produce osteoblasts and maintain its levels to produce new bone matrix (Clarke, 2008). The osteoprogenitor lineage regulates the expression of bone morphogenetic proteins (BMP) and Wingless (Wnt) proteins to induce differentiation of osteoblasts (Canalis et al. 2003). Osteoblasts are cuboidal cells that reside in the periosteum and endosteum and accounts to 4 to 6 % of all bone cells. They have a high amount of rough endoplasmic reticulum (RER), Golgi apparatus and secretory vesicles to produce proteins (collage) and secrete osteoid tissue in the matrix. The function of the osteoblasts is to produce new bone and; this involves several transcription factors Runt-related transcription factor 2 (RUNX2) gene, Osterix (Osx) and Distal-less homeobox that upregulates bone matrix proteins: osteocalcin (OCN), alkaline phosphatase (ALP) and bone sialoprotein (BSP) (Fukumoto and Martin, 2009; Marks and Popoff, 1988). It later becomes trapped in the calcified bone matrix where their structure and function alter from mature osteoblasts to form osteocytes; the most common form of bone cells (Ducy et al., 1997). This alters the ultrastructure of the cells and their size. The RER and Golgi apparatus decreases and the protein synthesis and secretion decreases (Schaffler et al. 2014). Osteocytes are situated in the lacunae in adjacent lamellae that form matrix channels (canaliculi) to create the central canal. The central canal consists of nerves and blood vessels that form a branched network called Volkmann's canals (perforating canal) and; this extends from the two membranes periosteum and endosteum and therefore; acts as a nutrient supply and removes waste products. This, in turn, supports the structure of the bone and the surface of the Quiescent bone lining cells (BLCs) (Clarke, 2008). It is important to state that the canaliculi are essential for the communication of osteoblasts and osteocytes because they do not undergo mitosis as opposed to the osteogenic stem cells that have mitotic activity. Osteocytes are metabolically active and secrete various enzymes and matrix proteins for adhesion and to maintain the mineral concentration in the calcified bone matrix. They also express OCN and a cell adhesion receptor called CD44 to produce a bone matrix protein called hyaluronate and this is essential for the structure and metabolism of the bone (OpenStaxCollege, n.d.). Furthermore, osteocytes secrete integral cellular proteins, for example, connexins maintain the gap junctions between bone cells. Gap junctions are required for maturation, activity, and survival of osteocytes (Clarke, 2008). Besides, osteocytes secrete lysosomes and can act as phagocytes (Clarke, 2008). BONE HOMEOSTASISBones are formed by the osteoblasts whereas; the osteoclasts dissolve the old proteinaceous matrix. This releases the calcium ions, repair, and remodels to form new osseous tissue. The osteocytes act as a mechanosensory stimulator for the bone-remodelling process and participate in the osteoblastic and osteoclastic activities (Florencio-Silva et al. 2015). Bone homeostasis is regulated by local and systemic factors: systemic factors include parathyroid hormones, calcitonin and oestrogen hormone whereas local factors include cytokines and growth factors (Florencio-Silva et al. 2015). Osteoclasts and osteoblasts are multinucleated bone cells that develop from mononuclear precursor cells of the monocyte-macrophage lineage (Clarke, 2008; OpenStaxCollege, n.d.). This is facilitated by two cytokines produced by marrow stromal cells: receptor activator of NF-κB ligand (RANKL) and the macrophage/monocyte colony-stimulating factor (M-CSF). RANKL belongs to the Tumour Necrosis factor (TNF) family are needed for the differentiation, proliferation, and survival of cells. M-CSF binds to its receptor c-Fms to stimulate the recruitment of adaptor proteins and cytosolic kinases to induce cellular signalling. There is crosstalk between M-CSF and RANKL, where M-CSF can stimulate the RANKL-RANK-OPG signalling pathway that regulates the production and maturation of the osteoclasts (Al-Bari and Al Mamun, 2020). OPG is a membrane-bound protein that prevents the association of RANKL with its receptor (Clarke, 2008; Al-Bari and Al Mamun, 2020). Overexpression of OPG causes osteopetrosis where there is a deficiency of the osteoclasts, however, when the deletion of OPG occurs, it causes overactivity of the osteoclasts leading to osteoporosis. Dysregulation of the remodelling process influences the calcium and phosphate homeostasis causing fracture, pain and deformity (Ralston, 2017; Yin et al., 2019). Another factor that stimulates osteoclastogenesis is tumour necrosis factor-related apoptosis-inducing ligand (TRAIL) receptors that activate TRAF6 and receptor activator of nuclear factor‐κB (NF‐κB) signalling pathways which upregulates the expression of nuclear factor of activated T cells cytoplasmic 1 (NFATc1) (Clark, 2008). Resorption of the bone is facilitated by hydrogen ions, metalloproteinases, cathepsin K enzyme and microtubules. Hydrogen ions are produced by the chloride channels and the enzyme H+ ATPases and; it acidifies the area of resorption that contains type I collagen. The B1 family of integrin receptors in the membranes of the osteoclasts binds to the peptides present in the bone matrix via the actin filament. This forms a sealed actin ring and; the matrix become polarised. Examples of peptides are laminin, fibronectin, osteopontin and sialoprotein. Resorption of the bone can be evaded if the actin ring is blocked. The resorbing osteoclasts transition into actin-containing podosomes that attach to the matrix (Clarke, 2008). Recent studies suggest that autophagic activity can affect bone homeostasis that can cause osteoporosis (Yin et al., 2019). Osteoblasts, osteoclasts and osteocytes have a basal level of autophagic activity where it contributes to their differentiation, functioning and survival in hypertonic, hypoxic and nutrition-deficient environments (Nollet et al. 2014; Zhu et al. 2017; Zheng et al. 2017; Dallas et al. 2013; Shapiro et al. 2014) BONE MARROWThe bone marrow is a soft, gelatinous, lymphoid tissue found in the medullary cavities of trabecular bone and there are two types: red bone marrow consists of haematopoietic/myeloid tissue and yellow bone marrow consists of adipose tissue surrounded by vascular sinuses and capillaries (Travlos, 2006; Allied academies, 2020). It is considered one of the largest organs in the body and accounts ~ 5% of the body weight. It is particularly found in the hip and thigh bones. A multidisciplinary approach can be performed to understand and evaluate the composition of the bone marrow through peripheral blood examination in toxicity studies, bone smears, iron stores, bone marrow aspirates and tissue sections through histological examination to determine alterations and architecture of the cells and tissues for inflammation and other pathological features (Travlos, 2006). The bone marrow has been mentioned in one of the hadiths narrated by Abu Hurairah (may Allah have mercy upon him) that Prophet (peace be upon him) said: “The first batch (of people) who will enter Paradise will be (glittering) like the full moon, and the batch next to them will be (glittering) like the most brilliant star in the sky. Their hearts will be as if the heart of a single man, for they will have neither enmity nor jealousy amongst themselves; everyone will have two wives from the houris, (who will be so beautiful, pure and transparent that) the marrow of the bones of their legs will be seen through the bones and the flesh." [Hadith, Al Bukhari, 3254] There are also haematopoietic and mesenchymal stem cells found in the bone marrow producing red blood cells (erythropoiesis), white blood cells (lymphopoiesis; granulopoiesis) and platelets (megakaryocytopoiesis). This maintains the self-renewal process of pluripotent stem cells and results in the differentiation and maturation of cells – the colony-forming unit is granulocytes, erythrocytes, monocytes, and megakaryocytes (CFU-GEMM) (Travlos, 2006) Many people with anaemia and blood cancers (leukaemia and lymphoma) rely on bone marrow or cord blood transplants to survive. When a disease outbreaks and affects the bone marrow, it causes the bone marrow not to function effectively. This is treated with marrow or cord blood transplant. Erythrocytes illustrated in Figure 6 are produced in the erythroblastic islands and are regulated by the humoral factor, erythropoietin that is primarily produced in the kidneys and small aliquots are found in the liver. Erythropoietin proliferates the progenitor cells and increases the differentiation and maturation of erythrocytes (Travlos, 2006). Erythropoiesis is also regulated by hormones of the gonads, adrenal, pituitary and thyroid glands. Growth hormone, androgens and thyroxine stimulate the production of erythropoietin. Oestrogen has an inhibitory effect that maintains the levels of erythropoietin (Karsten et al. 2018). The pro-inflammatory factors that are involved in erythrocytes are interferons (IFN-α2; IFN-γ); interleukins (IL-1α, -5, -9, -12, -15, -17 and -18), TRAIL, TNF and Macrophage migration inhibitory factor (MIF) (Karsten et al., 2018). The anti-inflammatory factors that are involved in erythrocytes are the following cytokines: IL-4,-10 and -13.  Figure 6: Erythrocytes Lymphopoiesis takes place in the bone marrow microenvironment whereas; T cell lymphopoiesis takes place in the thymus. There are heavy chains present in the pre-B cells that vary by size. The size of the smaller pre-B cells are ca. 9 microns and mature into B cells. The larger pre-B cells express A and K chains and are regulated by the stromal cells. Other cells are produced in other locations, for instance, granulocytes are synthesised in distinctive focis and platelets are produced adjacent to the endothelium (Travlos, 2006). Other cytokines are also involved in the regulation of cellular differentiation and maturation in the haematopoietic microenvironment. IL-2 and IL-3 produce macrophage and myeloid cells respectively. IL-3 also produces T lymphocytes. Burst promoting activity (BPA) is produced by T-lymphocytes and macrophages. Bone morphogenetic protein 6 (BMP-6) regulates chondrogenesis, osteogenesis and decreases osteoclastic differentiation via IL-6 (Hassan et al., 2004). Growth factors, for instance, basophils (CFU-Baso) megakaryocytes (CFU-Meg), erythrocytes (BFU-E) eosinophils (CFU-Eos) lymphocytes differentiate into progenitor cells in the bone marrow. Neutrophils and monocytes, on the other hand; rose from granulocyte-macrophage progenitor (CFU-GM) (Hassan et al., 2004). THE TYPES OF BONES MENTIONED IN THE QURAN AND HADITH.HEEL One of the bones mentioned in the Quran is the heel illustrated in Figure 7. Allah (The Most High) states: “My verses had already been recited to you, but you were turning back on your heels.!"[Quran, Surah Al Muminoon (The Believers), 23:66] The scholars mentioned concerning this verse that Allah (The Most High) called mankind but they refused and resisted in believing in Him (Ibn Kathir, 2000). From an anatomical perspective, the foot has three parts: forefoot, midfoot and hindfoot. The calcaneus (heel bone) is the largest tarsal bone in the hindfoot (AAOS, 2020). 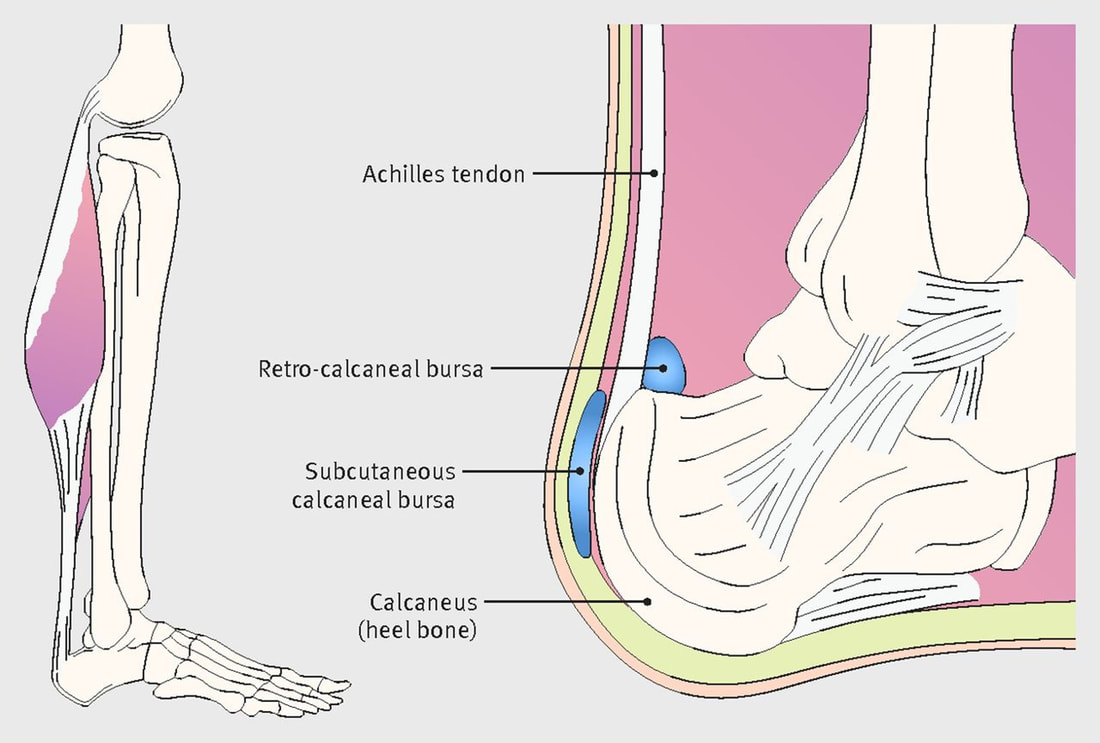 Figure 7: Anatomy of the back of the foot (Morton, 2016) CLAVICLE The clavicle (shoulder bone) is another type of bone mentioned in the Quran. Ibn Manzur (1993) mentioned about the following verse that the clavicle binds the neck to the shoulder region. “Yea, when (the soul) reaches to the collar-bone (in its exit).” [Quran, Surah Al Qiyamah (Judgement Day): 75:26]. Another reasoning narrated by Ibn Manzur (1993) is the presence of the two bones that associates the shoulder with the neck where the soul leaves the body between both clavicles during the death process. COCCYX The coccyx otherwise known as the tailbone; is a triangular bone that consists of 3 to 5 rudimentary coccygeal bounded segments in the terminal section of the vertebrae illustrated in Figure 8. The name is derived from the Greek phrase for a cuckoo bird's beak due to similar features (Lirette et al. 2014). The coccygeal cornu articulates the sacral cornua and is supported by the muscle: coccygeal gluteus maximus and; the ligaments - sacrotuberous and sacrospinous ligaments. The tendons on the lateral end are required for the bowel movement and supporting the pelvis during the seating posture that adds pressure to the coccyx (Lirette et al. 2014).  Figure 8: The anatomical structure of the vertebrae. The coccyx has been mentioned in many hadiths that are summarised in Table 1. It can withstand pressure and cannot be destroyed by the decaying process of the corpse. It is described as ‘ajbu azzanab’ meaning 'the end of the final part of something'. The primitive streak that develops in the embryo in the 3rd-week shrinks and remains in the sacrococcygeal region and the stem cells adheres (Yusof et al., 2016). This may explain as to why teratoma, tumours of the coccygeal origin have a combination of different tissues: skin, bones, cartilage, muscles and teeth in comparison to tumours of other regions (Yusof et al. 2016). This further suggests as to why the coccyx is reconstructed during Judgement day. Despite the teeth is found in the coccyx - it is not a bone. They share similar commodities with the bone, for instance, the hydroxyapatite content. There is much evidence in the Quran and Hadith of cleansing the tooth and its benefits. This is particularly with the miswak which is from the branches of the arak tree. This has been consolidated by research conducted by Winarni et al. (2019) where miswak has antimicrobial properties and can improve the periodontal health. There are also spiritual benefits of the miswak where it was related from Aisha (may Allah have mercy upon her) that the Prophet (peace be upon him) said: “The merit of the salat performed after using a miswak is seventy times of the salat performed without using a miswak.” [Ahmad bin Hanbal, Musnad, VI, 272]. However, this hadith is not clear because the Hanafi school states that the merit occurs by using the miswak whilst performing ablution. On the other hand, the school of Shafi states that merit occurs when using the miswak before the prayer. Furthermore, Allah (The Most High) states in the following verse: “They say what! When we are reduced to bones and dust, should we really be raised (to be) a new creation?” [Quran, Surah Isra (The Night Journey) 17:49] Ibn Manzur (1993) mentioned about the verse that the bones remain after death, whereas the muscles and the varied types of the tissue will decompose into dust. Other scholars such as Ibn Kathir (2000) mentioned that 'dust' is concerning the soil. This illustrates the rigidity of the bone. Mujahid (may Allah have mercy upon him) thought that the verse was about those who disbelieve where the resurrection will not be a place of denial. Ali bin Abi Talha (may Allah have mercy upon him) reported from Ibn Abbas it regarding dust (Al Tabari 17:464). But Allah (The Most High) responds in another verse that after disintegration, one can be resurrected. "But now they ask mockingly, “Will we really be restored to our former state, even after we have been reduced to decayed bones?" [Quran, Surah An-Naziat (Those who drag forth), 79: 10-11] In another verse, The Almighty states: "And they argue with Us—forgetting they were created—saying, “Who will give life to decayed bones?” [Quran, Surah Ya-Sin, 36:78] Say, "Be you stones or iron", or whatever you think is harder to bring to life!” Then they will ask ˹you˺, “Who will bring us back ˹to life˺?” Say, “The One Who created you the first time.” They will then shake their heads at you and ask, “When will that be?” Say, “Perhaps it is soon!” [Quran, Surah Isra (The Night Journey) 17:50-51] The scholars, Mujahid, Said ibn Jubayr, Abu Salih, Al-Hasan, Qatadah and Ad-Dahhak agree that creating a substance is not difficult for Allah and if one was dead, Allah can easily resurrect (Al Tabari, 17:463; Ibn Kathir, 2000). Table 1: Evidence of the coccyx in the hadith 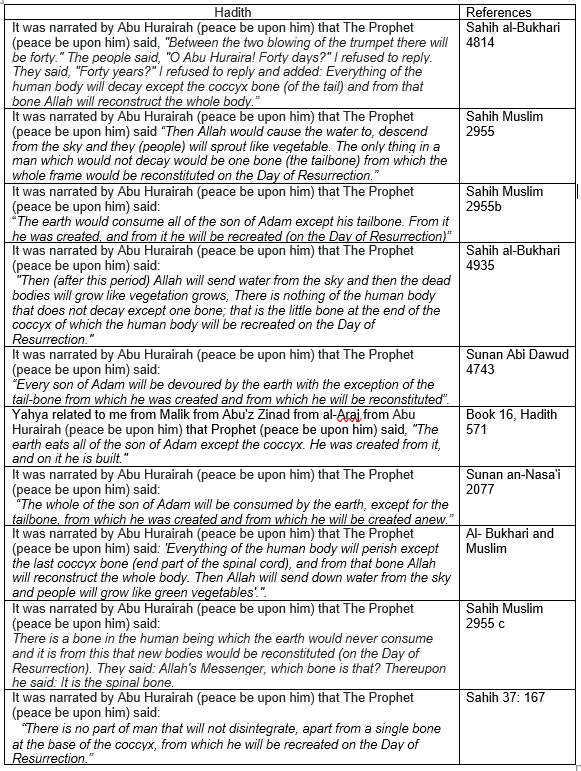 OTHER FEATURES OF THE MUSCULOSKELETAL SYSTEM JOINTS A joint combines two or more bones to aid in mobility. The main types of joints are fibrous, synovial and cartilaginous and are dependent on the type of tissue and movement. For instance, a fibrous or cartilaginous are connected by connective tissue and does not have a bone cavity. The fibrous joint is found in the sutures of the skull, and the gomphosis of the teeth. Cartilage joints reside in the intervertebral joints and the symphysis pubis. On the other hand, a synovial joint is situated in the knee has a bone cavity. They have synovial fluid to remove friction which decreases contact between bones. Other examples are shoulder, hip and elbow. There are several sub-types of synovial joints: the hinge joint, ball and socket and the gliding saddle (Al-Najjar, 2005). Gliding joints are present in the wrists where flat bone surfaces glide freely in several directions. In total, there are 360 movable joints in the human body. 147 joints in the vertebral column, 24 joints in the thorax, 86 joints in the upper extremity, 92 joints in the lower extremity and 11 joints in the pelvis. The vertebral column has 25 joints between the vertebrae and 72 joints between the vertebrae and the ribs. The thorax has two joints between the sternal bones and thoracic cage, 18 joints between sternum and ribs, 2 joints between clavicle and scapulae and 2 joints between scapulae and thorax. The upper extremity has 2 joints between the scapular bone, 6 joints between elbows, 8 joints between the wrists and 70 joints between the hand bones. The lower extremity has 2 hip joints, 6 joints between knee bones, 6 joints between ankles and 74 joints between feet bones. The pelvis has 4 joints between coccyx vertebrae, 6 joints between the acetabulum bones and 1 joint of the pubic symphysis (Al Najjar, 2012). The hadith that confirms the total number of joints are as follows:Aisha (may Allah have mercy upon him) narrated that the Prophet (peace be upon him) said: "Everyone has been created with three hundred and sixty Joints. Whoever mentions Allah's greatness (says Allahu Akbar), praises Allah, extols Allah, and seeks forgiveness from Allah and removes stones from the path of the people, enjoins what is good and forbids the evil to the amount of those three hundred and sixty joints (sulama), he walks on that Day (of Judgment) having distanced himself from the Hell fire." Isn't this miraculous that the Prophet Muhammad (peace be upon him) precisely knew the number of movable joints ‘salama’ that many in the subsequent centuries could not identify an accurate number and have given estimates between 200 and 300 joints? The joints have also been associated with acts of goodness, for instance, giving charity, seeking His remembrance and forgiveness and acts of charity and evading evil. Abu Dharr (may Allah have mercy upon him) narrated that the Prophet (peace be upon him) said: "In every morning there is a charitable act on the joints of any of you. Every tasbihah (to say: subhanallah, i.e. Glory be to Allah) is a charitable act; every tahmidah (to say: al-hamdu lillah, i.e. Praise be to Allah) is a charitable act, every tahlilah (to say: la ilaha illallah, i.e. There is none worthy of worship but Allah) is a charitable act; every takbirah (to say: Allahu akbar, i.e. Allah is the Greatest) is a charitable act; enjoining the right is a charitable act; forbidding the evil is a charitable act. However, to fulfill that charity, it is sufficient to pray two rak'at of Duha." [Sahih Muslim] This emphasises how mankind should be grateful to Allah for the ability to move via our joints to do good charitable acts and even pray to Allah (The Most High). Scholars such as Ibn Hajar Al Asqalani encouraged mankind to do charity because of the body's natural phenomenon. Furthermore, there are several references to the joints in the Quran, Allah (The Most High) states: “(Remember) when your Lord revealed to the angels, verily, I am with you, so keep firm those who have believed. I will cast terror into the hearts of those who have disbelieved, so strike them over the necks, and smite over all their joints.'' [Quran, Surah Al Anfal, 8:12] Ibn Manzur (1993) mentioned that the joints or 'banaan' are the small joints in the fingers or can be from the lower and upper limbs but the verse is about all joints because they can be dissociated easily. MUSCLES The muscles aid in mechanical movement and how the musculotendon work is independent of the total joint work that is the time that joint power over a full gait cycle (Sasaki et al., 2009). It has been described in the Quran as 'flesh' in 23:14. Three types of muscles are characterised by their morphological features and type of movement. Skeletal muscle is a voluntary muscle that controls body movement. The smooth muscle conducts movement involuntarily via the autonomic nervous system and can be found in the hollow viscera walls of the gastrointestinal tract and respiratory tract. The cardiac muscle is found in the heart within the myocardium and in the aorta and vena cava vessels. It conducts an involuntary movement which is also controlled by the autonomic nervous system. Page (2012) described the skeletal and cardiac muscles with striated features. The skeletal muscles have bundles of myofibres that contains myofibrils and sarcomere. The myofibres produce fascicles that create the muscle tissue where the extracellular matrix and cytoskeletal proteins encompass each muscle layer. Its function is to maintain energy metabolism and cellular homeostasis (Mukund and Subramaniam, 2019). Skeletal muscle comprises of the autonomic nerves to facilitate the transmission of impulses and has a regulatory framework to maintain cellular homeostasis and oxygen levels (Mukund and Subramaniam, 2019). Dysregulation of the muscle contraction can be caused by environmental stress, for instance, oxidative stress and inflammation that can cause fibrosis, hypertrophy and atrophy (Mukund and Subramaniam, 2019). The movement of the synovial joints is dependent on the range of motion (ROM), that involves the muscles and joints. The muscle serves as a tension mechanism where passive muscle tension depends on the fascia and viscoelastic properties whereas active tension occurs in dynamic muscles and have neuroreflexive properties that involve alpha and gamma motor neurons (Page, 2012). The contraction of the skeletal and cardiac muscles is achieved by the depolarization of the calcium ion voltage-gated channels that open in response to the action potential. The neurotransmitter is released and; the depolarization spreads whereby dihydropyridine receptors in the skeletal muscles increase calcium ions that bind to Troponin C to form a cross bridge. Myosin bind to the actin when tropomyosin moved. Adenosine diphosphate (ADP) is released that causes the muscle to contract. The myosin head is released where the cycle repeats (Shreshta, 2015) Similarly, for the smooth muscle to contract, action potential causes calcium ion voltage-gated channels to open. However, the calcium binds to calmodulin as opposed to Troponin C. The enzyme myosin light chain kinase is activated and, the myosin causes muscle contraction. bone tumoursAlterations in the cellular features of the bone and dysregulation of the bone homeostasis can cause tumorigenesis. Tumour cells can metabolically aid osteoblasts and osteoclasts to increase aggressiveness (Sousa and Clezardin, 2018). It is vital to understand the normal histological structure and function of the bone and; how the pathophysiological mechanisms develop to research and manufacture novel therapeutic interventions (Fornetti et al. 2018). Sarcomas are tumours of the connective and support tissues that occur in bone, blood vessels, cartilage and fat tissues. Bone sarcomas arise from mesenchymal cells and stromal cells (Cortini et al. 2019). Stromal cells facilitate the tumour development and are formed by osteoblasts, osteoclasts, immunological factors and mesenchymal stem (MSC) cells (Cortini et al. 2019, Tzelepi et al. 2000). MSC cells derived from the adult bone marrow can differentiate with a doubling time of two days where under culture conditions it is ca. 6 fold. They are positive for several immunological markers: CD29, CD166, CD44 and CS105 (Hassan et al. 2004). Amongst the malignant bone sarcomas are: osteosarcoma, Ewing sarcoma and chondrosarcoma that account to 70% of malignancies causing high rates of mortality and morbidity presented in Figure 9 (Rajani and Gibbs, 2012). The patient survival rate of bone sarcomas has improved due to presence of combinational (adjuvant) chemotherapy after tumour resection in the 1970s and 1990s; but cases are still high (Fornetti et al. 2018; Simpson et al. 2018). There is a high risk of drug resistance following chemotherapy and; this can lead to the development of metastasis in the lungs that is characterised by poor prognosis. The development of the tumours in the bone will be incurable and undergo palliative care. A combinational approach between doxorubicin and methotrexate or cisplatin can be achieved where ca. 70% with no metastasis whereas with metastasis ca. 20% (Rajani and Gibbs, 2012). Osteosarcomas arise in the juxtaepiphyseal region and medullary cavities in the metaphysis of long bones where it rapidly grows in the arms and legs. The primary bone tumour primarily occurs in children aged 10 to 25 and is the third most common cancer amongst children and adolescents after lymphomas and brain cancers (Wang et al., 2018). It is characterised by the presence of the osteoid tissue and irregular and disorganised structure of the bone caused by malignant MSC cells (Simpson et al. 2018; Picci, 2007). Osteosarcoma can be subdivided based on clinical, histological and radiographic evidence: Intramedullary (low-grade) and surface (high-grade) (Misserschmit et al. 2009). Intramedullary osteosarcoma comprises of the destruction of the cancellous and cortical bone with the soft tissue extension. There are ca. 2% of osteoid tissue present in the diaphysis and metaphysis of long bones that can be misinterpreted to the benign lesion or fibrous dysplasia (Rajani and Gibbs, 2012). It is treated with neoadjuvant chemotherapy. Periosteal sarcoma are chondroblasts where some osteoid tissue are formed (Rajani and Gibbs, 2012) The pathophysiology of osteosarcoma is not well understood, however, the genetic factors have primarily contributed to tumorigenesis and tumour development. It can occur sporadically because of mutations in genes that encode for the proteins involved in the cell cycle regulation (Misaghi et al. 2018; Wang et al. 2018). For instance, Inactivation of the tumour suppressor genes; p53 and retinoblastoma (RB) and overexpression of MDM2 can cause bone tumour cells to proliferate. Mutations in the chromosomal number 17p13 can cause Li Fraumeni syndrome and the uncontrolled proliferation of cells are apparent (Simpson et al. 2018; Lietke et al. 2014). Additional alterations can occur in the BLM and RECQL4 genes that encode DNA helicases who function in unwinding the double-stranded DNA for replication – this leads to genetic syndromes such as Bloom and Rothmund-Thomson syndrome (Simpson et al. 2018). Staging of the tumour involves local and distant radiographical imaging of the destruction of the bone and the medullary bone soft tissue. Magnetic Resonance Imaging (MRI) presents the neurovascular structures and the metastasis, whereas the CT scan presents the pulmonary metastasis that occurs in the lungs. Response to chemotherapy can be determined by the Positron Emission Tomography (PET) (Rajani and Gibbs (2012). Other diagnostic radiological imaging used to evaluate the tumour are dynamic bone scintigraphy and angiography. To confirm the diagnosis of osteosarcoma, a biopsy is also requested (Picci, 2007). This presents progress in the diagnostic methods for osteosarcoma. Furthermore, amputation was commonly performed in the past, however; the survival rate was minimal in comparison to today where treatment is more advanced (Picci, 2007). Today, ITAP implants occur in patients with amputations. Besides, mTOR inhibitors (mammalian target of rapamycin) inhibitors were used for combinational therapy. mTOR is a phosphatidylinositol 3’ kinase (PI3K) serine-threonine that phosphorylates downstream signalling pathways to induce DNA repair and increase cellular proliferation. Also, the PI3K/AKT/MAPK pathway is also influenced by the insulin-like growth factor. 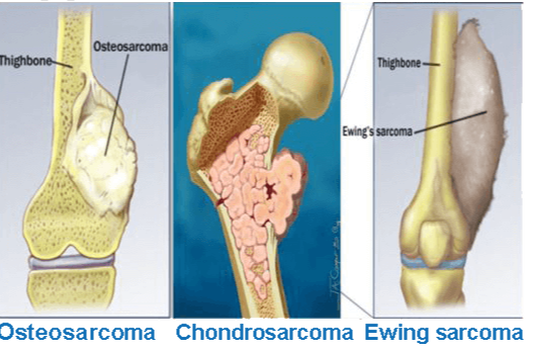 Figure 9 - Examples of bone tumours EWING SARCOMA The following osteosarcoma is the most common paediatric malignancy and is characterised by round blue cells. Ewing sarcoma is caused by the chromosomal translocation (11;22)(q24;q12) that encode the EWS/FLI oncoprotein to maintain the malignant phenotype (Rajani and Gibbs, 2012; de Alava et al. 2013). To diagnose Ewing Sarcoma, it requires a range of molecular diagnostic methods to detect fusion genes of ETS family, histological and immunological techniques (Osaki, 2015; Delattre et al. 1992). Recent studies using the electron microscope and immunohistochemistry techniques suggests it has a neurogenic origin (Osaki, 2015). The standard treatment for Ewing Sarcoma is intense neoadjuvant and adjuvant chemotherapy (Osaki, 2015). This is normally doxorubicin, vincristine, etoposide, cyclophosphamide, ifosfamide and actinomycin-D (Osaki, 2015). There can also be a combined therapeutic approach which has proven effective: vincristine, doxorubicin and cyclophosphamide with radiation and surgery (Rajani and Gibbs, 2012). CHONDROSARCOMA Conventional chondrosarcomas account for most of the incidence of chondrosarcoma. They are mesenchymal tumours that affect the cartilage cells in the craniofacial and can also initiate in the intramedullary cavities of the femur, pelvis, shoulder, hip and, ribs (Rajani and Gibbs, 2012). Dedifferentiated chondrosarcomas occur in the chondroid areas of the pelvis and long bones and account for ca. 10% of chondrosarcomas (Boehme et al. 2018). Secondary chondrosarcomas, for instance, enchondromas, develop from cartilage lesions. Peripheral chondrosarcomas are caused by benign paediatric bone tumours called osteochondromas. Clear cell chondrosarcomas are rare low-grade tumours that occur in the epiphysis in the bone (Boehme et al., 2018). Chondrosarcoma is caused by the Hedgehog signalling and alterations in p53 and RB genes that affect the cell cycle regulation, migration, proliferation, angiogenesis and; other hallmarks of cancer (Rajani and Gibbs, 2012). Furthermore, chondrosarcoma cells are characterised by the loss of primary cilia which is caused by histone deacetylase 6 (HDAC6) which in turn induces tumour proliferation (Boehme et al., 2018). It is treated with chemotherapy. OTHER BONE TUMOURS Osteomas are benign tumours caused by the chromosomal alteration of 5 and can also cause Gardener's syndrome. Tumours arising in the skull, femur, tibia and vertebrae. Leiomyosarcoma occurs in the blood and organs. Leiomyomas reside in the fibroids and the lining of blood vessels in uterine cells. Rhabodomyomas soft tissue sarcoma develops in the voluntary muscles, nerves, fat, blood vessels, cartilage and bones in the head, neck and gastrointestinal tract of paediatric patients. Giant cell tumours have a soap bubble appearance and affect long bones and joints in the thighbone (femur) and shinbone (knee joint). This highlights there is a range of different types of bone tumours and recent studies have shown that 3D culture models are a novel approach in investigating tumour cells and its microenvironment to module the paracrine response, resistance to tumour drugs and the aggressiveness of tumours than rodent models (Cortini et al., 2019). Overall, the bone is an interesting source and the structure, function and physiology have been presented in the Quran, Hadith and literature work. Despite, the Quran is not a scientific book, it continues to serve as a fundamental purpose and guidance alongside the Mustalahul Hadith (authenticity of the hadith) where some of its verses provide scientific evidence that is progressively unrevealed by modern medical and scientific research. Next month, it will be the last section of my research project; where I will discuss the anatomy and physiology of the intestines and; the evidence found in the Quran and Hadith. The muscle in the intestinal wall aids in the digestion and absorption of food. Furthermore, Zhang et al. (2018) revealed that the intestinal microbial flora has a functioning role in bone health whereby it can dysregulate bone homeostasis by evading osteogenesis and inhibiting osteoblastic and osteoclastic activity by upregulating genes and growth factors that alter the hormones that play a role in the bone metabolism, for instance, cortisol, androgens and serotonin and this in turn; affects the bone mass. REFERENCESAAOS (2020) Calcaneus (Heel Bone) Fractures Available [online] https://orthoinfo.aaos.org/en/diseases--conditions/calcaneus-heel-bone-fractures/
Ahmad, Y. (2010) Islamic medicine: A key to better life. Saudi Arabia: Darussalam. Al‐Bari, A. and Al Mamun, A., (2020) Current advances in regulation of bone homeostasis. FASEB BioAdvances, 2(11), pp.668-679. Al-Hakim, S. (1968) al-Mustadrik alá al-Sahihayn fi al-hadith. wa-fi dhaylihi Talkhis al-Mustadrik. Egypt: Maktabat wa-Matabi al-Nasr al-Hadithah Allied Academies (2020) Bone Marrow Articles Open Access. Available [online] https://www.alliedacademies.org/scientific-journals/bone-marrow-articles-open-access-16112.html Al-Najjar, Z. (2005) Wonderful Scientific Signs in the Qur’aan UK: Al Hijaz Al-Tabari, A. (2001) Tafsir Al Tabari: Jami Al Bayan An Ta'Wil Aayi al Qur'an. USA: Darussalam. Boehme, K., Schleicher, S., Traub, F. and Rolauffs, B., (2018) Chondrosarcoma: A Rare Misfortune in Aging Human Cartilage? The Role of Stem and Progenitor Cells in Proliferation, Malignant Degeneration and Therapeutic Resistance. International Journal of Molecular Sciences, 19(1), p.311. Canalis, E., Economides, A. and Gazzerro, E., (2003) Bone Morphogenetic Proteins, Their Antagonists, and the Skeleton. Endocrine Reviews, 24(2), pp.218-235. Clarke, B., (2008) Normal Bone Anatomy and Physiology. Clinical Journal of the American Society of Nephrology, 3(Supplement 3), pp.S131-S139. Cortini, M., Baldini, N. and Avnet, S., (2019) New Advances in the Study of Bone Tumors: A Lesson From the 3D Environment. Frontiers in Physiology, 10.814. Creative Biomart (2020) ‘Skeletal development Proteins’ Available [online]:https://www.creativebiomart.net/researcharea-skeletal-development-proteins_819.htm Dallas, S., Prideaux, M. and Bonewald, L., (2013) The Osteocyte: An Endocrine Cell … and More. Endocrine Reviews, 34(5), pp.658-690. De Alava, E., Lessnick, S.L. and Sorensen, P.H., Ewing Sarcoma (2013) In: Fletcher, C.D.M., Bridge, J.A., Hogendoorn, P.C.W., Mertens, F., editors. WHO classification of tumours of soft tissue and bone. Lyon: WHO Press. pp. 305–309. Delattre, O., Zucman, J., Plougastel, B., Desmaze, C., Melot, T., Peter, M., Kovar, H., Joubert, I., de Jong, P., Rouleau, G., Aurias, A.and Thomas, G. (1992) Gene fusion with an ETS DNA-binding domain caused by chromosome translocation in human tumours. Nature. 359(6391):pp.162–165. Ducy, P., Zhang, R., Geoffroy, V., Ridall, A.L., and Karsenty, G. (1997) Osf2/Cbfa1: a transcriptional activator of osteoblast differentiation. Cell. 89(5) pp. 747-754. Eriksen, E.F., Axelrod, D.W. and Melsen, F. (1994) Bone Histomorphometry, New York: Raven Press, pp1 –12. Fawwaz, Z. (1999) Al-Durr Al-Manthur fi Tabaqat Rabbat Al-Khudur Beirut: Dar al-Kutub al-Ilmiyah; al-Tabah. Fornetti, J., Welm, A. and Stewart, S., (2018) Understanding the Bone in Cancer Metastasis. Journal of Bone and Mineral Research, 33(12), pp.2099-2113. Florencio-Silva, R., Sasso, G., Sasso-Cerri, E., Simões, M. and Cerri, P., (2015) Biology of Bone Tissue: Structure, Function, and Factors That Influence Bone Cells. BioMed Research International, 2015, pp.1-17. Fukumoto, S., and Martin, T.J. (2009) Bone as an endocrine organ. Trends in Endocrinology and Metabolism 20 (5), pp. 230-236. Hassan, H. and El-Sheemy, M., (2004) Adult bone-marrow stem cells and their potential in medicine. JRSM, 97(10), pp.465-471. Ibn Hatim Tafsir Al-Quran Al-Azim Saudi Arabia: Maktaba Nizar Al-Baz. Ibn Kathir (2000) Tafsir Ibn Kathir. Saudi Arabia: Darussalam. Ibn Manzur, M. (1993) Lisan Al-Arab Beirut: Dar Ihyaa Al-Turath Al-Arabi. Imster, E. (2019) A few favorite snowflake photos Available [online] https://earthsky.org/earth/best-snowflakes-photos-from-earthsky-friends Karsten, E., Breen, E. and Herbert, B.R. (2018) Red blood cells are dynamic reservoirs of cytokines. Scientific Reports 8, 3101. Lirette, L. S., Chaiban, G., Tolba, R., & Eissa, H. (2014). Coccydynia: an overview of the anatomy, etiology, and treatment of coccyx pain. The Ochsner journal, 14(1), 84–87. Luetke, A., Meyers, P.A., Lewis, I. and Juergens, H., (2014) Osteosarcoma treatment – where do we stand? A state of the art review. Cancer Treatment Reviews. 40(4): pp. 523-532. Marks, S.C. and Popoff, S.N. (1988) Bone cell biology: the regulation of development, structure, and function in the skeleton. American Journal of Anatomy, 183 (1), pp. 1–44. Messerschmitt, P.J.; Garcia, R.M; Abdul-Karim, F.W; Greenfield, E.M and Getty, P.J. (2009) Osteosarcoma, Journal of the American Academy of Orthopaedic Surgeons: 17(8) – pp. 515-527 Misaghi, A., Goldin, A., Awad, M. and Kulidjian, A., (2018) Osteosarcoma: a comprehensive review. SICOT-J, 4, p.12. Moore, K. L. and Persaud, T. V. N. (1998) The developing human: clinically oriented embryology. 6th ed. Philadelphia: Elsevier Saunders. Morton, S., Newth, A. and Majeed, A., (2016) Pain at the back of the heel. BMJ, p.i1366. Mukund, K. and Subramaniam, S., (2019) Skeletal muscle: A review of molecular structure and function, in health and disease. Wiley Interdisciplinary Reviews: Systems Biology and Medicine. 12(1): e1462 Nollet, M., Santucci-Darmanin, S., Breuil, V., Al-Sahlanee, R., Cros, C., Topi, M., Momier, D., Samson, M., Pagnotta, S., Cailleteau, L., Battaglia, S., Farlay, D., Dacquin, R., Barois, N., Jurdic, P., Boivin, G., Heymann, D., Lafont, F., Lu, S., Dempster, D., Carle, G. and Pierrefite-Carle, V., (2014) Autophagy in osteoblasts is involved in mineralization and bone homeostasis. Autophagy, 10(11), pp.1965-1977. OpenStaxCollege, (n.d.) ‘Bone Structure’ Available [Online]: http://pressbooks-dev.oer.hawaii.edu/anatomyandphysiology/chapter/bone-structure/ Page P. (2012). Current concepts in muscle stretching for exercise and rehabilitation. International journal of sports physical therapy, 7(1), 109–119. Picci, P., (2007) Osteosarcoma (Osteogenic sarcoma). Orphanet Journal of Rare Diseases, 2(6). Qutb, S., and Salahi, A. (2015) In the Shade of the Qur'an (Fi Zilal al-Qur'an): Surah 33 Ahzab - Surah 39 Al-Zumar: v. 14 UK: The Islamic Foundation. Rajani, R. and Gibbs, C., (2012) Treatment of Bone Tumors. Surgical Pathology Clinics, 5(1), pp.301-318. Ralston, S., (2017) Bone structure and metabolism. Medicine, 45(9), pp.560-564. Sadler, T. W. (2010) Langman's medical embryology.11th ed. Philadelphia: Lippincott William & Wilkins. Sasaki, K., Neptune, R. and Kautz, S., (2009) The relationships between muscle, external, internal and joint mechanical work during normal walking. Journal of Experimental Biology, 212(5), pp.738-744. Schaffler, M.B., Cheung, W-Y., Majeska, R., and Kennedy, O. (2014) Osteocytes: master orchestrators of bone. Calcified Tissue International 94(1), pp. 5-24. Scheuer, L. and Black, S. (2000) Developmental juvenile osteology. London: Elsevier Science. Shapiro, I. M., Layfield, R., Lotz, M., Settembre, C. and Whitehouse, C. (2014) Boning up on autophagy: the role of autophagy in skeletal biology. Autophagy 10, 7–19. Shrestha, S. (2010) Mechanism of Skeletal Muscle Contraction Available [online] https://medchrome.com/basic-science/physiology/mechanism-of-skeletal-muscle-contraction/ Simpson, E. and Brown, H., (2018) Understanding osteosarcomas. Journal of the American Academy of Physician Assistants, 31(8), pp.15-19. Travlos, G., (2006) Normal Structure, Function, and Histology of the Bone Marrow. Toxicologic Pathology, 34(5), pp.548-565. Tzelepi V., Tsamandas A.C., Zolota V., Scopa C.D. (2009) Bone Anatomy, Physiology and Function. In: Kardamakis D., Vassiliou V., Chow E. (eds) Bone Metastases. Cancer Metastasis – Biology and Treatment. 12, pp 3-30 Wang, L., Gebhardt, M. and Rainusso, N. (2018) Osteosarcoma: epidemiology, pathogenesis, clinical presentation, diagnosis, and histology. Available [online] www.uptodate.com/contents/osteosarcoma-epidemiology-pathogenesis-clinical-presentation-diagnosis-and-histology Winarni, Y., Haslinda, R. and Aspalilah, A., (2019) Miswak: The underutilized device and future challenges. Journal of Dentistry and Oral Hygiene, 11(2), pp.6-11. Wyganowska-Świątkowska, M. and Przystańska, A., (2010) The Meckel’s cartilage in human embryonic and early fetal periods. Anatomical Science International, 86(2), pp.98-107. Yin, X., Zhou, C., Li, J., Liu, R., Shi, B., Yuan, Q. and Zou, S., (2019) Autophagy in bone homeostasis and the onset of osteoporosis. Bone Research, 7(1). Young, B., Lowe, J. S., Stevens, A and Heath, J. W. (2006) Wheather’s functional histology: a text and colour atlas. 5th ed. Philadelphia: Churchill Livingstone Elsevier. Yusof, N., Che, N., Che, A. and Hassan, A. (2016) The anatomy of the musculoskeletal system in the light of Al Quran and hadith. In: 2nd World Congress on Integration and Islamicisation: Focus on Medical and Healthcare Science (2WCII 2016), 21st-23rd October 2016, Kuantan, Pahang. Zhang, J., Lu, Y., Wang, Y., Ren, X. and Han, J., (2018) The impact of the intestinal microbiome on bone health. Intractable & Rare Diseases Research, 7(3), pp.148-155. Zheng, L., Wang, W., Ni, J., Mao, X., Song, D., Liu, T., Wei, J. and Zhou, H., (2017) Role of autophagy in tumor necrosis factor-α-induced apoptosis of osteoblast cells. Journal of Investigative Medicine, 65(6), pp.1014-1020. Zhu, L., Chen, J., Zhang, J., Guo, C., Fan, W., Wang, Y. and Yan, Z., (2017) Parathyroid Hormone (PTH) Induces Autophagy to Protect Osteocyte Cell Survival from Dexamethasone Damage. Medical Science Monitor, 23, pp.4034-4040.  On the 5th of November, we discussed the association between the evidence from the two foundations of Islam: the Quran and Sunnah with the anatomy and physiology of the brain. The Quran and Prophetic traditions consist of religious, spiritual, scientific, medical and anatomical texts that act as a guide (Loukas et al., 2010). It is natural for me to discuss my favourite book, the Glorious Quran as a Muslim to research and contemplate on the beauty of its words and the wisdom behind its meanings. This section of the project aims to discuss the structure and function of one of the most vital organs in the body that has a strong relationship with the brain and; that is the heart. The heart is amongst the infinite blessings from Allah (The Most High) and; as we observe and analyse the various functions of the organs within the human body, we continuously contemplate the creativity and kindness of Allah (The Most High) in how they function 24 hours and 7 days a week. Allah (The Most High) states in the Glorious Quran: "And if you should count the favours of Allah, you could not enumerate them. Indeed, Allah is Forgiving and Merciful." [Quran, Surah Al-Nahl (The Bee), 16:18] Over the centuries, clinical researchers have understood the impact that various anatomists, philosophers and artists have contributed to the gross anatomy of the heart from the ‘Father of Medicine’ Hippocrates to Galen to Leonardo Da Vinci (Roberts et al., 2019). Advances in understanding the structure and function in the post-Hippocratic era were about the interconnection between the lungs and the heart via the pulmonary circulation. The unsung hero, Ibn Al-Nafis made significant contributions to the earlier knowledge about the pulmonary circulation during the Islamic Golden age forming the link between Galen with scholars of the Rennaissance era: Michael Servetus, Realdus Columbus, Andreas Vesalius and William Harvey (West, 2008). However, how many of you knew it was the Quran that was revealed more than 14 centuries ago that initially provided humanity with the factual knowledge on the heart and the pulmonary circulation and their vitality in the maintenance of life? Allah (The Most High) states: "Created man from a clinging substance." [Quran, Surah Al-Alaq (The Clot), 96:2] The 'clinging substance' or 'alaq' refers to the formation of a leech-like clot of blood from the uterine wall during the embryonic stage. Later in the developmental stages, it forms the pulmonary circulation where the heart has not started beating because it has developed the distinctive characteristics (Aga, 2020). Therefore, the summary of literary works from the initial research on the cardiovascular system to its maturation and the framework of the Quran and Hadith provide evidence on the cellular, molecular and enzymatic levels. This provides an insight into the mechanisms that occur in the normal and abnormal circulation of the heart. Lancellotti et al. (2020) revealed that abnormal circulation and injury to the anatomical structures of the heart can lead to cardiovascular diseases and even tumours. Both diseases are the predominant causes of high mortality rates globally. Tumours of the heart are rare and are diagnosed as benign. Myxoma is the most common type that occurs in the left atrium of most paediatric patients but can in some cases occur in the right atrium. Rhabdomyoma is more of an advanced type of cancer and is linked with Tuberous sclerosis (National Institute of Cancer, 2009). Another example of a malignant tumour is angiosarcomas that is highly pleomorphic in nature even with immunohistochemistry. It is treated with neoadjuvant therapy (chemotherapy or radiotherapy) to shrink the tumour size before removing the micrometastases via surgery (National Institute of Cancer, 2009). Cardiotoxicity is one of the complications following cancer treatment and; this can cause autonomic dysfunction where there is variability in the heart rate and, it can also lower the cardiorespiratory fitness levels which affect the prognosis and survival rates of cancer patients (Grote et al., 2020). Grote et al. (2020) further added that when cancer patients conduct combined aerobic and resistance training (CART) at home or using minimal resources, it improves the fitness levels and maintain the sinus rhythm. The Glorious Quran positions the heart at a lofty position from two respects: the physical and spiritual perspectives for intention, faith and understanding (Olatoye, 2013). From a physical perspective, the heart is a hollow muscular organ that pumps blood around the body via the circulatory system. It approximately beats 72 times per minute throughout our lives, this is ca. 4.7 – 5.7 litres of blood per minute. It approximately weighs 250 to 400 and 300 to 350 grams in the female and male respectively (Marieb and Hoehn, 2015). The function of the heart is to carry glucose, oxygen, amino acids, metal ions (sodium, calcium and potassium) to conduct vital functions, for instance: muscule contraction and homeostasis (Marieb and Hoehn, 2015). The blood also removes waste products which we do require for instance; carbon dioxide. Within the spiritual context, Allah (The Most High) refers to the heart as its ability to process emotions, sentient, make intentions, actions, moral values, making the decision, and reasoning and intellectually suggesting its fundamental relationship between the heart and mind (Olatoye, 2013). Allah (The Most High) describes the heart 132 times in the Quran using three phrases: Qalb, Sadr (44 times) and Fuad (16 times) (El-Najjar, 2005). Qalb is derived from the word ‘qalaba’ which is the nature of the heart that can change something or turn it around (Loukas et al. 2010). Respected scholars such as Al-Ghazali (2005) reported that the Qalb refers to the physical and spiritual heart and; both require to be kept sound and healthy to operate. This relates to the following hadith where our Beloved Prophet (peace be upon him) refers the heart in a metaphorical sense and states: “Truly in the body, there is a morsel of flesh which, if it is sound, all the body is sound and which, if it be diseased, all of it is diseased. Truly it is the heart.” [Hadith, Al-Bukhari, Muslim] Other scholars such as Ibn Taimiyyah (1998) stated regarding this hadith that the heart is the commander and the limbs are the soldiers that follow. If the heart is good, the soldiers are good and; if the heart is evil; then the soldiers become evil and; it is important to love things only for Allah (The Most High). Another scholar, Ibn Hajer Al-Asqalani (2004) described the heart as singled out because it is the leader of the body in which through purification of the leader, the subjects become purified and when corruption occurs they become corrupted (Olatoye, 2013). Sadr refers to the chest or breasts that entails the secrets where Allah (The Most High) states: “Who whispers [evil] into the breasts of mankind” [Quran, Surah Al-Nas, 114:5] Fuad refers to the heart as an organ that processes emotions, for example, when the mother of Prophet Moses (peace be upon them) had to put her newborn Moses in the river to protect him from the evil actions of the Pharoah. But there came to be a void in the heart (Fuad) of the mother of Musa. [Quran, Surah Al-Qasas, 28:10] Therefore, understanding the structure and function of the heart aids in diagnosing and treating cardiac diseases. The spiritual heart can be infected, for instance, sadness and anger; this affects the soul; whereas the physical heart can affect the body with disease. Advances in 3D imaging can be utilised to observe the segmented sections of the cardiac anatomy without influencing the relationship into the intrathoracic structures (Mori et al. 2019). The anatomy and physiology of the heart The heart is a muscle that contracts and expands rhythmically and involuntarily. It is situated within the mediastinal cavity of the thorax between the right and left lung which; extends posteriorly to the second and fifth intercostal muscle as presented in Figure 1 (Jarvis and Saman, 2018). The main function of the heart is to pump blood around the body in conjunction with blood vessels using the Cardiac cycle where the heartbeats 72 times per minutes. It has a helical and circumferential structure to aid in its mechanical activity (Buckberg et al. 2018). Buckberg et al. (2018) discovered that the cardiac dynamics influences the movement of the cardiac muscle in particularly the left ventricle, right ventricle and septum where narrowing, lengthening, twisting, shortening, uncoiling and widening occurs. The heart consists of layers: the outer layer is the pericardium which prevents it from overexpanding the thorax and is attached to the inner sternal surface in the anterior end and diaphragm at the posterior end. It is subdivided into two layers: fibrous layer which contains a dense layer of connective tissue and the serous pericardium also, known as the epicardium (Jarvis and Saman, 2018). The serous fluid separates both of the pericardial layers to provide a smooth motion. The middle layer is the myocardium that comprises of cardiomyocytes (cardiac muscle cells) and; the inner layer is known as the endocardium (Jarvis and Saman, 2018).  Figure 1: The location of the heart within the chest cavity. Inside the heart, there are four compartments called a chamber - Figure 2. The upper chamber is called the atrium whereas; the lower chamber is called the ventricle. Each side of the heart has two chambers and; there is a thick muscular wall called a septum that separates the right and left side of the heart. The left ventricle has a circular cavity with a thicker wall in comparison to the right ventricle that has a crescent cavity and thinner wall (Marieb and Hoehn, 2015). The presence of the four cardiac valves prevents the backward flow of the blood. The valves have cusps (projections) where the chordae tendinae (tendons) are bound with the inner cardiac walls by papillary muscles.  Figure 1: The anatomical structure of the heart (Franklin Institute, 2020) The blood and the pulmonary circulation Amongst the cells found in the blood are red blood cells (erythrocytes) that carry oxygen to each cell around the body. They contain a red pigment called haemoglobin that covalently binds with oxygen to form oxyhaemoglobin. The red blood cells carry oxygen into the cells where it utilised and; carbon dioxide is carried away from the blood. The artery blood vessel carries blood away from the heart and; the veins carry blood back to the heart. This movement of blood is called circulation where; it is estimated that it takes 60 seconds to pump blood to each cell. The arteries are divided into smaller blood vessels called arterioles and then even smaller branches called capillaries. The veins are divided into smaller blood vessels called venules. The right atrium receives deoxygenated blood from the inferior and superior vena cava as presented in Figure 3. The deoxygenated blood from the head and neck is via the superior vena cava whereas; the inferior vena cava receives deoxygenated blood from the rest of the body. This then flows into the right ventricle. The tricuspid valve separates the right atrium and ventricle and has three cusps. Its function is to allow the deoxygenated blood to flow through (Marieb and Hoehn, 2015). The right ventricle pumps the deoxygenated blood through the pulmonary trunk into the lungs where it collects the oxygen molecules. The gas exchange particularly takes place in the alveoli of the lungs. The pulmonary trunk consists of left and right pulmonary arteries. The pulmonary valve separates the right ventricle and the pulmonary artery and this allows the flow of deoxygenated blood to enter the lungs (Marieb and Hoehn, 2015). The oxygenated blood is returned to the heart where it enters the left ventricle via the pulmonary vein. This explains why the left ventricular wall is thicker to withstand the pressure of oxygenated blood. The bicuspid valve also; known as the mitral valve has two projections and; it allows the flow of oxygenated blood from the left atrium to the left ventricle (Marieb and Hoehn, 2015). From the left ventricle, there is an aortic valve where the oxygenated blood flows through into the aorta and; this is transported around the body (Marieb and Hoehn, 2015). To summarise, the bicuspid and tricuspid valves function in the flow of the blood from the atria to the ventricles whereas; the aortic and pulmonary valves function in regulating the flow of blood leaving the heart. Concerning the evidence found in the Quran, the blood has been mentioned in terms of menstruation, the blood of animals, embryology and lineage. Allah (The Most High) states: "And We have already created man and know what his soul whispers to him, and We are closer to him than [his] jugular vein." [Quran, Surah Qaf (Letter Qaf), 50:16] This illustrates that the close distance of Allah (The Most High) to oneself is more important than the close distance of the blood vessel more than the importance of this blood vessel. The jugular vein is divided into interior and exterior and functions in returning deoxygenated blood from the brain, face and neck to the heart via the superior vena cava. Another evidence of the blood vessel in the Quran is in the following verse: "And if Muhammad had made up about Us some [false] sayings, We surely would have seized him by his right hand (or with power and might), And then We certainly would have cut off his life artery.” [Quran, Surah al-Haqqah (The Reality) 69:44-47] The scholars have mentioned that Al-Watin is the ‘aorta’ or an artery where if Prophet Muhammad (peace be upon him) lied about the teachings of Islam, the vital artery would be cut. From a positive aspect, it is in reference that the blood is the vehicle of life and survival based on the exegesis (Abdel Haleem, 2005). In relation to menstruation, it is advised to not do sexual intercourse nor prayer because of impurity and the ability to transmit pathogens via the blood causing infection. And they ask you about menstruation. Say, "It is harm, so keep away from wives during menstruation. And do not approach them until they are pure. And when they have purified themselves, then come to them from where Allah has ordained for you. Indeed, Allah loves those who are constantly repentant and loves those who purify themselves." [Quran, Surah Al Baqarah (The Cow) 2:222] There is another type of circulation and that is through the coronary arteries. It arises from the openings of the aorta called the coronary ostia and is situated in the epicardium and myocardium (Marieb and Hoehn, 2015). Its function is to supply the heart with oxygenated blood. The left coronary artery goes through the left side of the heart and is subdivided into the left circumflex and descending arteries. The right coronary artery goes through the right side of the heart and is subdivided into the marginal and posterior arteries (Marieb and Hoehn, 2015). Approximately two-thirds of the venous blood returns to the heart, in particular, the right atrium via a structured network of coronary veins called the coronary sinus that varies in types: small, middle, large and oblique, marginal and posterior veins. The last third of the venous blood enters the right atrium directly via the anterior cardiac veins (Marieb and Hoehn, 2015).  Figure 3: The pulmonary and system circulations The regulation of the heart The heart is regulated by the conduction system and the cardiac cycle. At first, the atria and ventricles relax in a coordinated manner; this is called diastole. To generate an electrical impulse, it requires a sequence of excitation that takes place in the cardiac muscle cells. There are two nodes: sinoatrial (SAN) and atrioventricular (AV) and these are specialised tissues that aid in the electrical activity of the heart. The SAN is situated in the right atrium and sets the sinus (heart) rhythm to initiate the electrical impulse following the contraction of the myocardium as presented in Figure 4. This then enters the atrium to contract (atrial systole) and is transmitted to the AV node that resides in the inter-atrial septum. This is done via three atrial internodal tracts: the left atrium via the Bachman’s bundle to the AV node, the middle internodal tract where there is the Wenckebach Bundle and; this flows from the septum to the AV node to conduct different speeds. The third way is from the posterior Internodal tract otherwise; known as the Thorel’s tract and; this occurs from the lower septum of the AV node. There is a minimal delay of 0.1 seconds of the AVN because of its smaller size and; this gives enough time for the atria to contract and fill 70% of the ventricles. The blood filling the ventricles is called the end-diastolic volume. The electrical impulse subsequently goes to the intraventricular septum to induce ventricular contraction (ventricular systole) whilst the atria relax and; this occurs via the insulated fibres called Bundle of His at the apex of the heart. The Bundle of His are subdivided into left and right bundles and contain papillary muscles. The non-insulated fibres: Purkinje fibres resides in the ventricular myocardium and travel into the right and left ventricles. The ventricles contract as the pressure increases and; this pushes the blood out of the aortic and pulmonary valves via the aorta arteries. The diastolic phase then occurs again and; this is where the ventricles relax as the ventricular pressure descends and; this causes the aortic and pulmonary valve to close. The remaining blood in the chambers is called the end of the systolic volume also; known as the isovolumetric relaxation. The diastole, atrial systole and ventricular systole events form the cardiac cycle - Figure 4 (Marieb and Hoehn, 2015). Furthermore, several chemicals affect the contractility of the heart, for instance, adrenaline and thyroxine – catecholamine and hormone respectively to induce a positive inotropic effect. On the other hand, calcium channel antagonists can have a negative inotropic effect on the heart (Marieb and Hoehn, 2015).  Figure 4: The regulation and coordination of the heart The heart from a spiritual perspective Despite my research project focuses on the anatomy and physiology of the heart, understanding how the heart and mind particularly the hypothalamus conjugate together to facilitate emotions, reasonings, the understanding of actions by intentions and acceptance of knowledge centralises their purpose within human nature. It can be Shubahat (level of understanding) or Shahawat (self-desire that grow out of proportion)(Loukas, et al. 2010). Allah (The Most High) states: "Truly it is not the eyes that become blind but do the hearts which are in the chests" [Quran, Surah Al-Hajj, 22: 46] Many researchers have discovered that there is a strong correlation between the heart and the brain. Previously in this project, we have covered the six senses and; these are considered external areas whereas; emotion is considered internal and; both forms are required to facilitate feelings and bridge the mind and heart (Sempo et al., 2017). The Glorious Quran particularly influences the sound and sight senses. Many Quranic verses and Hadith use the terms: 'in the heart' and 'from the heart' to describe the cardiac state. The good heart is of the Al-Muminoon (The Believers) and; it connotates happiness, gratitude, faithful, love, gentleness mercy, a balanced rational and other positive traits. It is a heart that fears and loves Allah (The Most High) and remembers Him through supplication, worship, seeking repentence and using each moment wisely in preparation for the Hereafter (Afterlife). It is free from Shahawat and relies on Allah (The Most High) - Nafs Al Mutmainah - a satisfied soul (Tahmasebi, 2015; Olatoye, 2013). It was narrated that Abu Hurairah (May Allah have mercy upon him) reported that our Beloved Prophet Muhammad (peace be upon him) said: "People whose hearts are like the hearts of birds will enter Paradise". [Hadith, Muslim, 2840] In reference to this hadith, Al-Nawawi (may Allah have mercy upon him) stated it means that they are those who rely upon Allah (The Most High) and have soft hearts. The second type of heart is referred by the scholars as bad or dead hearts of the Non-Believers. This is due to their harshness, acts of aversions, arrogance, suspicion, sins and other negative traits. It has no life and follows worldly pleasures. It is the Nafsul Ammarh - a commanding soul (Tahmasebi, 2015; Olatoye, 2013). The third type of heart is the diseased or sick hearts of the hypocrites who have feelings of emptiness, weakness and are terrified. They harbour between the good and bad heart where there is the love of Allah (The Most High) and is also dead because of the desires - Nafsul Lawwammah (the complaining soul) (Olatoye, 2013). Ibn Qayyim Al-Jawziyyah (2000) has described the diseased heart with not feeling pain when sinning, finding pleasure when disobeying Allah, not influenced by admonition, lack of prioritisation of what is important, difficulty in accepting the truth and a feeling of discomfort amongst righteous believers. Our Beloved Prophet (peace be upon him) made the following supplication (dua) and was narrated by Ibn Umar (may Allah have mercy upon him): "O’ Allah, I seek refuge in you from a heart without conscious fear of Allah, a prayer unanswered, an unsatisfied soul, and knowledge with no benefit. I seek refuge in You from these four things!" [Hadith, Al-Nasai, 43] This emphasises the diseased heart has no conscious fear of Allah (The Most H igh). Besides, El-Najjar (2005) gave an additional type of heart and; it is the heart that reasons with its ability to process thinking, rewarding, reasoning and punishment. A summary of some of the Quranic evidence of the types of hearts can be found in Table 1. Table 1: The Quran evidence on the different types of heart  The heart influences the brain and the rest of the body neurologically via the nervous system, biophysically through the pulse waves and electromagnetically via the energetic waves (Loukas et al., 2010). Its strong rhythm branches out the electromagnetic field and; it is sensed by every cell of the body processing information - this is known as the heart code (Pearsall, 1999). The heart has been described by Tahmasebi (2015) as a cognitive tool that hears the words of Allah, maintaining faith and performance of righteous acts to fulfil our divine purpose. Allah (The Most High) states: "Those who have believed and whose hearts are assured by the remembrance of Allah. Unquestionably, by the remembrance of Allah hearts are assured." [Quran, Surah Al Raad (The Thunder), 13:28] This suggests how the Quran (The Most High) can provide a healing status on the nervous, hormonal and immune system. Many studies emphasise how stress and pessimism is an independent risk factor that can stimulate the inflammatory process causing hypertension and coronary heart disease (Kurd et al. 2013; Vale, 2005). On the other hand, people with an optimistic vision and good lifestyle management strategies are calm. It was reported by Pearsall et al. (2005) that following peripheral organ transplants such as the heart, it affects the behaviour and personality traits that are proportional to the donor and this is because of the systemic memory and decider subsystems in place. This is a similar case with kidney and liver where sensations change towards food, and emotional factors are linked with the donor's history (Joshi, 2011). However, these transitional changes could be caused by immunosuppressant drugs, stress and psychopathology of the donors (Pearsall et al. 2005; Joshi, 2011). Allah (The Most High) states: "Did We not expand for you, [O Muhammad], your breast?" [Quran, Al-Sharh (The Relief), 94:1] Many of the scholars agreed that this is a metaphorical reference about Allah (The Most High) opening the heart of Prophet (peace be upon him) about Islam, faith and knowledge in the reports of Al-Bukhari and Al-Basri in their commentaries of Surah Al-Sharh. Ibn Ashur (2000) further suggests that this is in reference to the levels of perfection and blessings upon him from Allah (The Most High) because Allah is pleased with him. Ibn Uthaymeen (may Allah be pleased with him) mentioned in his Tafseer that the opening of the heart is related to the decree of Allah (The Most High) in terms of religion and the calamities or trials that man faces. Ibn Kathir (1988) reported that this verse is similar to the following verse: "So whoever Allah wants to guide - He expands his breast to [contain] Islam; and whoever He wants to misguide - He makes his breast tight and constricted as though he were climbing into the sky. Thus does Allah place defilement upon those who do not believe." [Quran, Surah Al-Anaam (The Cattle) 6:125] On the other hand, other scholars mentioned that this is about the surgical opening of the heart that occurred twice where there are hadiths concerning the events when he was small and the other during the night of Israa (The night Journey). It was narrated from Anas ibn Malik (may Allah have mercy upon him) that Jibreel (may Allah be pleased with him) came to Prophet Muhammad (peace be upon him) when he was playing with the other boys in the Banu Saad tribe. He took hold of him and threw him to the ground, then he opened his chest and took out his heart, from which he took a clot of blood and said: “This was the Shaytan’s share of you.” Then he washed it in a vessel of gold that was filled with Zamzam. Then he put it back together and returned it to its place. The boys went running to his mother – meaning his nurse – and said: Muhammad has been killed! They went to him and his colour had changed. Anas said: I used to see the mark of that stitching on his chest. [Hadith, Muslim, 162] Abu Dharr narrated that Prophet (peace be upon him) said: “The roof of my house was opened when I was in Makkah, and Jibreel (may Allah be pleased with him) came down and split open my chest, then he washed it with Zamzam water. Then he brought a golden basin filled with wisdom and faith and emptied it into my chest. Then he sealed it." [Al-Bukhari; 349 and Muslim; 163] Ibn Al-Hajar Al-Asqalani (2004) mentioned that some scholars disagree that the open heart surgery took place during the night journey and only occurred when Prophet (peace be upon him) was young. However, he and Al-Qurtubi (1996) added there is various strong evidence that suggests the second event did occur and should not be objected. The ultimate point of mentioning this event is that following this incident, Prophet (peace be upon him) had a significant change in his outward approach towards Islam and belief. Ramadan and the cardiac patient Ramadan is the holy month for Muslims where they fast from dawn until sunset and perform good deeds (Chamshi-Pasha, 2013). It is put forward ca. 10 days before the previous year. Amongst those exempt are the elderly, the pregnant, breast-feeding, very young children, those who are travelling and the unwell, for instance, people with heart disease and diabetes. Allah (The Most High) states: "O you who have believed, when you rise to [perform] prayer, wash your faces and your forearms to the elbows and wipe over your heads and wash your feet to the ankles. And if you are in a state of janabah, then purify yourselves. But if you are ill or on a journey or one of you comes from the place of relieving himself or you have contacted women and do not find water, then seek clean earth and wipe over your faces and hands with it. Allah does not intend to make difficulty for you, but He intends to purify you and complete His favor upon you that you may be grateful." [Quran, Surah Al-Maidah (The Table), 5:6] However, a few studies have revealed that there are positive effects of fasting in cardiac patients. Temizhan et al. (1999) compared patients with acute coronary heart disease and unstable angina before, during and after Ramadan and discovered that the mortality rates decreased in Ramadan in comparison to prior or post-Ramadan (p=0.03). However, amongst the limitations of this study is that the sample population size was small (1655) to discover whether there was a significant difference. On the other hand, Salim et al. (2013) reported no significant difference between before and after fasting Ramadan. There were no alterations in the blood pressure, body mass index and lipid profile of patients with stable cardiac illness wherein the latter there was 30-40% improvement in the level of high-density lipoproteins. However, diabetic patients must be monitored (Salim et al., 2013). Another study revealed that intermittent fasting that includes restricting the number of calories help improve the cardiovascular and neural function via the neurotrophic factor signalling pathway in the brain which increases sensitivity to insulin and lowering the blood pressure (Mattson and Wan, 2005). These findings can lead to the discovery of novel therapeutic modalities. However, the effect of fasting varies with each patient and should comply with optimised treatment and dietary needs. Pilgrimage and the cardiac patient When Muslims go on the annual pilgrimage (Hajj) that takes place in Makkah, several symptoms can occur in patients with heart disease, for instance, thirst, sun exposure and communicable diseases such as respiratory infections (Chamsi-Pasha, 2013). This is why the patient must consult their General Practitioner (GP) before the journey to do a health check, ensure there is a compliant supply of medications and provide the necessary advice. Avoiding crowds is also a preventative measure to prevent cardiac decompensation (Chamsi-Pasha, 2013). A recent study by Yilmaz et al. (2019) discovered that there was a significant difference in the number of times medicines were used before and after Hajj (pilgrimage) (p=0.011). However, in the three-month follow up, there was no difference nor complaints after Hajj (p=0.094). This suggests how the treatment compliance differs with the period of time wherein the short-term interval there is a negative effect whereas; in the long-term, it is positive or has no difference (Yilmaz et al., 2019). There are many ways of how to take care of the heart from a spiritual and physical sense and; that is through lifestyle management, praying and type of food. The Muslim prayer is a combination of standing, sitting and prostrating and; the units of prayer varies with each prayer. Loukas et al. (2010) informed that the movements of prayer helps digest food and stimulate the leg muscles gastrocnemius and soleus to increase the return of venous blood to the heart when standing and displaces the blood from the two veins: peripheral and central veins to prevent oedema and decrease the formation of a thrombus (Loukas et al., 2010). Furthermore, it is understood that Muslims do not eat the meat of the pigs and; there is scientific reasoning behind this. There is high level of fat and contain Trichinella parasite that can cause infection (Vasilev et al. 2012). Besides, healthy food, for instance, talbina (barley) is recommended for cardiac patients. Overall, the Quran and Hadith have significant revelations on the physical and spiritual concepts of the heart more than 14 centuries ago and this facilitates in seeking knowledge on nature at an exponential rate in combination with the literature, particularly, the anatomy and physiology of various organs of the body forming a clear consensus. This section of the project leads us to subsequently discuss next month, the anatomy and physiology of the bone where the red blood cells that carry oxygen in the blood around the body are made.  Figure 5: An insight of the red and white blood cells in the bone. References Abdel Haleem, M.A.S (2005) The Qur’an: A new translation. UK: Oxford University Press.
Aga, M., (2020) It Was The Qur'an That First Revealed The Fact Of Blood Circulation In Human Body. Available [online] https://www.missionislam.com/science/blood.html Al-Ghazali, M. (2005) Ihya Ulumud-Din. Egypt: Dar Al-Ghad Al-Gadeed. Al-Najjar, Z. (2005) Wonderful Scientific Signs in the Qur’aan UK: Al Hijaz Al-Qurtubi, A.I. (1996) Al-Mufhim. Syria: Dar Kalam Al Tayib. Buckberg, G., Nanda, N., Nguyen, C. and Kocica, M., (2018) What Is the Heart? Anatomy, Function, Pathophysiology, and Misconceptions. Journal of Cardiovascular Development and Disease, 5(2), p.33. Chamsi-Pasha, H. (2013) Islam and the cardiovascular patient – pragmatism in practice. British Journal of Cardiology 20:90. Franklin Institute (2020) Structure of the heart. Available [online] https://www.fi.edu/heart/structure-heart Grote, S., Ricci, J.M., Dehom, S., Modeste, N., Sealy, D-A., Tarleton, H.P. (2020) Heart Rate Variability and Cardiovascular Adaptations Among Cancer-Survivors Following a 26-Week Exercise Intervention. Integrative Cancer Therapies. Ibn Ashur (2000) Tafsir al Tahrir wal Tanwir. Ibn Al-Hajar Al-Asqalani (2004) Fath Al-Bari bi Sharh Sahih Al-Bukhari. Cairo: Dar al-Hadith. Ibn Kathir, (1988) Tafsir Al-Quran Al-Azim Egypt: Dar al-Misriyah al-Lubnaniyah Ibn Qayyim al-Jawziyyah (2000) The Invocation of God (Al-Wabilu ‘l Sayyib mina ‘l-Kalimi ‘l-Tayyib), UK: Islamic Texts Society Ibn Taimiyyah (1998), Diseases of the Hearts and their Cures. Birmingham: Al-Hidayah Publishing and Distribution. Jarvis S. and Saman, S (2018) Cardiac system 1: anatomy and physiology. Nursing Times [online]; 114: 2, 34-37. Joshi, S. (2011) Memory transference in organ transplant recipients. 19 (1) Journal of New Approaches to Medicine and Health. Kurd, B.J., Dar, M.I., Shoaib, M, Malik, L., Aijaz, Z., and Asif, I. (2014) Relationship between stress and coronary heart disease. Asian Cardiovascular and Thoracic Annals. 22(2) pp. 142-147. Lancellotti, P., Mai-Linh Nguyen Trung, M-L., Oury, C. and Moonen, M. (2020). Cancer and cardiovascular mortality risk: is the die cast?, European Heart Journal, ehaa871. Loukas, M., Saad, Y., Tubbs, R.S., and Shoja, M.M. (2010) The heart and cardiovascular system in the Qur’an and Hadeeth. International Journal of Cardiology; 140: 19-23. Marieb, E., and Hoehn, K., (2015) Human Anatomy and Physiology. 10th ed. UK: Peason. Mattson, M.P. and Wan, R. (2005) Beneficial effects of intermittent fasting and caloric restriction on the cardiovascular and cerebrovascular systems. Journal of Nutritional Biochemistry. 16(3) pp. 129-37. Mori, S., Tretter, J., Spicer, D., Bolender, D. and Anderson, R., (2019) What is the real cardiac anatomy?. Clinical Anatomy, 32(3), pp.288-309. National Cancer Institute (2009) Matters of the Heart: Why Are Cardiac Tumors So Rare? Available [online] https://www.cancer.gov/types/metastatic-cancer/research/cardiac-tumours. Olatoye, R.M., (2013) Towards understanding the Islamic concept of the heart and its relationship with man’s intentions/actions. 1st Annual International Interdisciplinary Conference. Portugal. Pearsall, P. (1999) The Heart’s Code: Tapping the Wisdom and Power of Our Heart Energy. UK: Broadway Books. Pearsall, P., Schwartz, G., and Russek, L. (2005) Organ Transplants and Cellular Memories. Nexus Magazine 12 (3). Roberts, W., Salandy, S., Mandal, G., Holda, M., Tomaszewksi, K., Gielecki, J., Tubbs, R. and Loukas, M., 2019. Across the centuries: Piecing together the anatomy of the heart. Translational Research in Anatomy, 17, p.100051. Salim, I, Al Suwaidi, J., Ghadban, W., Alkilani, H. and Salam, A.M. (2013) Impact of religious Ramadan fasting on cardiovascular disease: a systematic review of the literature. Current Medical Research Opinions 29 pp. 343–54. Sempo, M., Salam, R., Mohd, R., Zainudin, W., Zainol, Z., Zaki, Z., Ibrahim, M. and Sayuti, M., (2017) The Quranic Philosophy on Superiority of Audio Sense Against Visual Sense Based on the Book of Exegesis and Science Reports. Advanced Science Letters, 23(5), pp.4765-4768. Tahmasebi, Z., Abshenasan. M. and Karim, R. (2015). The concept of heart in Quran. Journal of Applied Environmental and Biological Sciences.5(10S); pp. 386-391 Temizhan, A., Donderici, O., Oguz, D. and Demirbas, B. (1999) Is there any effect of Ramadan fasting on acute coronary heart disease events? International Journal of Cardiology. 70 pp. 149-53. Vale, S., (2005) Psychosocial stress and cardiovascular diseases Postgraduate Medical Journal 81, pp. 429-435. West J. B. (2008). Ibn al-Nafis, the pulmonary circulation, and the Islamic Golden Age. Journal of applied physiology (Bethesda, Md: 1985), 105(6), pp. 1877–1880. Yilmaz, F., Sabanciogullari, S. and Karabey, G. (2019) The effect of Hajj Pilgrimage on Treatment Compliance in Individuasl with Chronic Diseases. Journal of Religion and Health 58, pp. 599-611. The brain is an organized and structured network with highly complexed functions and thousands of neurons created by Allah (The Most High). Amongst the functions are the six senses: sight, smell, proprioception, touch, taste and hearing covered last month where the brain receives nerve impulses via neurons from the sensory organs. Regardless of the human's technical, knowledge and power, a brain cannot be re-created and this is due to the resistance and signaling mechanisms it encompasses and was described by Penfield as a small universe. The aim of this article is not to provide extensive detail on the anatomy and physiology of the brain but to merely interconnect the verses from the Glorious Quran that associates it with understanding the anatomical-functional of the brain. Allah (The Most High) states: “This is the creation of Allah. So show Me what those other than Him have created. Rather, the wrongdoers are in clear error.” [Quran, Surah Luqman, Verse 11] “And He gave you from all you asked of Him. And if you should count the favor of Allah , you could not enumerate them. Indeed, mankind is [generally] most unjust and ungrateful.” [Quran, Surah Ibrahim, 14:34] “And if you should count the favors of Allah , you could not enumerate them. Indeed, Allah is Forgiving and Merciful.” [Quran, Surah Nahl, 16:18] The malfunction of the neural structure of the brain can cause tumours, injuries and other consequences. Tumours of the brain arise from neoplasms in the meninges and intracranial tissues. The incidence of brain tumours accounts for 2% of all cancers where there are more than 130 types of brain tumours (McKinney, 2004). Tumours can be differentiated based on the histological subtype, grade, stage, biology, presenting symptoms and prognosis and; this influences the type of treatment. The main type of brain tumour is supratentorial that occurs in the frontal, temporal and parietal lobes. Examples of tumours of the glia are glioblastoma, oligodendroblastoma and astrocytoma which increases with age but is less able to be detected in the elderly due to comorbidity conditions, for instance, strokes (Cancer Research UK, 2020). The main modalities of cancer treatment for glioblastomas and lymphoma are radiotherapy, chemotherapy, and surgery (Minniti et al. 2017). However, high doses of ionising radiation decrease the quality of life and increase the risk of neurological toxicity that is secondary to comorbidity (McKinney, 2004). Originally, radiation has been used as a single agent therapy but had little effect on the survival rates. However, an optimal administration of radiotherapy is required for co-adjuvant treatment with chemotherapy, but requires informed clinical decision making and design of randomized trials. This highlights the multidisciplinary approach to create an effective treatment paradigm for patients with brain tumours. Bonner et al. (2020) revealed that silencing of the Microtubule actin crosslinking factor 1 (MACF1), a cytoskeletal protein has anti-tumour properties for patients with glioblastomas where it increases the specificity of radiosensitization, decreasing the viability and migration of glioblastoma cells and impairing translational regulatory processes. There are two types of brain tumours: primary and secondary. Primary tumours of the central nervous system (CNS) initiate in any area of the brain where it can be benign or malignant (LaPointe et al. 2018). Benign tumours are within a defined area and; patients are less likely to have a remission following treatment; whereas malignant tumours can progress to other areas of the brain. Each year, 12100 primary tumours are diagnosed, and this includes the spinal cord, meninges and neurones (nerves) leading to the brain (Cancer Research UK, 2020). Tumours of the brain and spinal cords affect adult and children and; it is the second most common type of paediatric tumours in the UK but is more common in the elderly where it is estimated that for every 100 patients who are 75 or older, 25 people are diagnosed with brain or spinal tumours (Cancer Research UK, 2020). Secondary tumours grow faster and are much difficult to treat with a 5-year overall survival rate (LaPointe et al. 2018). According to statistics, there are 5500 people in the UK diagnosed with malignant cancers (Cancer Research UK, 2020). Gliomas are the most common malignant tumours that occur in adults (LaPointe et al. 2018). The introduction of molecular and genetic markers in the health service has improved prognosis and characterisation of tumours more accurately. Boudreau et al. (2005) revealed that genetic alterations, for instance, IDH, 1p/19q codeletion, RELA-fusion and H3 Lys27Met can be combined with histological techniques in the WHO classification of CNS tumours which aids in the understanding of the diagnosis and treatment of brain tumours. Advanced techniques, for instance, cytological staining and histopathological technology can provide a basis to understand neuroanatomy and increase the specificity of tumour diagnosis. Radiological diagnostic techniques, for instance, positron emission tomography (PET) measures the cerebral blood flow whereas, functional magnetic resonance imaging (MRI) and computed tomography (CT) can be used to understand the structure and function of the brain in response to the cognitive, motor and sensory tasks where the regional and laminar distribution of the human cerebral cortex can be observed (Marshall and Morriss-Kay, 2004). This is needed to complement with an understanding of the model systems to increase detection rates, improve the differential diagnosis of brain tumours that have previously been differentiated as stroke or metastatic tumours (McKinney, 2004). The delivery of care to cancer patients is also influenced by geographical differences, in the UK, cancer treatment is more advanced, and patients have long-term survival. However, the survival rate of brain tumours is low in comparison to other cancers and; there are also differences in its subtypes. For instance, meningiomas, have a better prognosis whereas; patients with glioblastoma multiforme (GBM) have the poorest survival in all age groups. The causes of brain tumours One of the risk factors of brain tumours is the accumulation of genetic alterations caused by chemical, physical and biological factors that evade regulatory mechanisms of neuronal cells and destruct the immune system. Genetic predisposition, for instance, tuberculosis, neurofibromatosis 1 and 2 and nevoid basal cell carcinoma syndrome and mutations of the Guardian of the Genome, p53 gene that can cause Li Fraumeni syndrome has been linked with gliomas (McKinney, 2004). It has also been reported that genes involved in cellular metabolic processes, for instance, DNA stability and repair, detoxification and oxidation can cause brain tumours (McKinney, 2004). Environmental carcinogens such as transplacental N-nitroso compounds (ethyl and methyl nitrosourea) that can cross the blood-brain barrier can have a dual effect. Dietary and environmental N-Nitroso compounds can induce tumours and can have an anti-oxidant effect where it can be found in fruits and vegetables. (McKinney, 2004). However, there are inconsistent reports made on the association between the constituent of the tobacco smoke, hair products, pesticides, pollution with the incidence of tumours and solvents (McKinney, 2004). This requires further research. The role of prokaryotes such as retrovirus and adenovirus have different putative roles causing brain tumours and is caused by the difference in the viral DNA sequences (McKinney, 2004). However, other viruses that cause influenza and varicella (chickenpox) have been linked with brain tumours but; this varies with the seasonality (McKinney, 2004). This suggests that the role of immunological factors in infections and the causation of brain tumours requires further research (LaPointe et al. 2018). The anatomy and physiology of the brain. To gain an accurate understanding of the anatomical-functional perspective of the brain, neuroimaging, electrophysical and; lesion studies have been conducted. The brain forms part of the central nervous system alongside the spinal cord and cranial nerves. The peripheral system consists of spinal nerves that stem from the spinal cord and the autonomous nervous system. The brain is a complex organ that comprise billions of organs and whose weight differs between a man and woman where it is 1336 grams and 1198 grams respectively, however, the difference in weight has no impact on intelligence nor function (Jawabli and Sharma, 2019). There are three fundamental areas in the brain: cerebrum, cerebellum and the brainstem with defined and precise functions as illustrated in Figure 1. The soul dominates the brain and; the soul understands the signals transmitted. Allah (The Most High) states: “Allah is˺ the One to Whom belongs the kingdom of the heavens and the earth, Who has never had ˹any˺ offspring, nor does He have a partner in ˹governing˺ the kingdom. He has created everything, ordaining it precisely.” [Quran, Surah Al-Furqan, 25:2]. The cerebrum contains the main portion of the brain and consists of two cerebral hemispheres. The longitudinal fissure divides the left and right hemispheres, whereas; the corpus callosum connects the lower area of the brain. The brain is composed of two types of cells: neurons and glial cells where the former transmits nerve impulses or signals whereas glial cells are non-neuronal cells that provide support in transmitting the signals from one neurone to another. It contains a myelin sheath that provides insulation. Other functions are maintaining homeostasis and nutrition (Baum et al. 2020). Together, the glial cells, neurons and; the cerebrum forms the human cerebral cortex. Allah (The Most High) states: So which of the favours of your Lord would you deny? [Quran, Surah Al Rahman, 55: 37-38] The cerebral cortex is the outer layer of the cerebrum that extends from the unimodal sensory cortex to the transmodal association cortex (Baum et al. 2020). It consists of grey matter and is fundamental for consciousness and neuronal computations, for instance, voluntary movement memory, communication, thought and; perception (Marguelis et al. 2016). It is anchored in the lower area of the brain by the white matter that comprises of fibres between neurons whose function is to coordinate neural activity (Baum et al. 2020). Additional features of the cerebral cortex consist of grooves of various sizes that are separated by bulges called gyri. This is where nerve impulses move from one gyrus to another and lobe to lobe. Small grooves are called sulci and the larger grooves are called fissures (Baum et al. 2020).  Figure 1: Annotation of the brain (Hoffmann, 2019) The cerebrum is divided further into lobes where each cerebral hemisphere consists of frontal, temporal, parietal and occipital that have a specialised function that complements one another. Therefore, malfunction or injury or a tumour arising can influence the ability to communicate. For instance, if one cannot speak, then it will influence their ability to read. Transmission of nerve impulses influences the motor cortex, where the left side would cause the right side of the body to move (Gilbert-Jaramillo et al. 2019). The frontal lobe contains five neural centres and is situated in the pre-frontal cortex behind the forehead. It is required to think, make sound decisions, memory, use of initiative, character, personality, behaviour, and truthfulness (Gray, Warwick and Williams, 1980; Jawabri and Sharma, 2016). There are different types of memories in which the brain processes and in the case of the frontal lobe, it focuses on the prospective memory which involves planning daily to long-term goals (Neulinger et al., 2016). The ability to make sound decisions involves the three aspects: learning, reasoning and creativity (Collins and Koechlin, 2012). The first neural centre in the frontal lobe is the motor speech area of Broca situated in the posterior inferior frontal gyrus (Flinker et al. 2015). It functions in the production and coordination of voices alongside the pharynx, larynx, tongue, and face (Baum et al. 2020). The primary motor area is situated in the posterior area to the precentral sulcus where it controls the voluntary muscle movement of the left side of the body whereas, the secondary motor area controls the voluntary muscle movement of the right side of the body (Chouinard and Paus, 2006). The frontal eye fields control the movement of the eyes. The fifth function is the frontal area that can control and direct evil actions, lying and deteriorate moral principles that are transmitted from the sensory organs to the effectors. The same verse from the Glorious Quran is reflected upon again where Allah (The Most High) states: So which of the favours of your Lord would you deny? [Quran, Surah Al Rahman, 55: 37-38] Yang et al. (2007) revealed that the pre-frontal cortex contains white matter where there is ca. 23-36% orbital frontal middle and inferior gyri but not superior and frontal gyri present in people who live than the normal controls. The rate of white matter is increased in those who pathologically lie (Yang et al. 2007). However, this has already been stated in the Glorious Quran by Allah (The Most High) where He states: “No! If he does not desist, We will surely drag him by the forelock - A lying, sinning forelock.” [Quran, Surah Al Alaq, 96:15-16] Scholars such as Keith Moore in a conference in 1980 confirmed that the frontal lobe of the brain functions in making informed decisions and direct human behaviour. The fronted bone in the skull protects the frontal lobe/forelock, direct human behaviour and make decisions. In a hadith, Prophet (peace be upon him) mentioned a supplication (dua) about the forelock, He said: There is no-one who is afflicted by distress and grief and says (the above), but Allah will take away his distress and grief, and replace it with joy.” He was asked: “O Messenger of Allah, should we learn this?” He said: “Of course; everyone who hears it should learn it: Oh Allah, I am Your servant, the son of Your servant, the son of your maid-servant, and entirely at Your service. You hold me by my forelock. Your Decree is what controls me, and Your Commands to me are just. I beseech You by every one of Your Names, those which You use to refer to Yourself, or have revealed in Your Book, or have taught to any one of Your creation, or have chosen to keep hidden with You in the Unseen, to make the Qur’an Al-Karim the springtime of my heart, the light of my eyes, the departure of my grief, and the vanishing of my affliction and my sorrow. [Ahmad 1:391, Ibn Hibban] This highlights the importance of the frontal lobe in guiding behaviour and is accountable for the deeds of man and; this is where we prostrate (sujood). Allah (The Most High) states: “Recite, [O Muhammad], what has been revealed to you of the Book and establish prayer. Indeed, prayer prohibits immorality and wrongdoing, and the remembrance of Allah is greater. And Allah knows that which you do.” [Quran, Surah Anqabut, 29:45] The cerebellum is the largest area of the hindbrain and approximately weighs 150g (Singh, 2020). It is separated by the cerebrum by a structure called the tentorium and is situated at the back of the brain below the occipital lobe. The cerebellum consists of functional gradients from the primary motor area to the transmodal regions. The other principal axis initiates from task unfocuses to task-focused regions (Guell et al. 2018). The main function of the cerebellum is to maintain the balance of the voluntary movements of the muscles and limbs, strength, and the contraction force (Singh, 2020). The nerve impulses are sent from the cerebral cortex to the spinal cord via the brainstem whereas; the cerebellum connects with the brainstem via the cerebellar peduncles (Singh, 2020). Other functions of the cerebellum include muscle tone and posture (Singh, 2020). The brainstem is situated in the lower extension of the brain, in front of the cerebellum and is connected to the spinal cord as presented in the MRI scan of the brain in Figure 2. There are three structures present in the brainstem and consists of grey and white matter: the pons (metencephalon), midbrain (mesencephalon), and the medulla oblongata (myelencephalon). The brainstem predominantly regulates the central nervous, respiratory and cardiovascular systems as well as the sleep cycle (Siacca et al. 2019). An additional function of the brainstem is to control consciousness by the reticular activating system. The function of the medulla oblongata is to monitor breathing, blood circulation, and heart rhythm. The midbrain and the pons functions in the ocular motion where the pons has additional functions such as facial sensation and movement, hearing and balance. This is led by the twelve cranial nerves that have specific functions: eye movement (oculomotor, trochlear, abducens), ability to see (optic), movement of the neck and shoulder muscles (accessory), taste sensations (glossopharyngeal, vagus), tongue movement (hypoglossal), hearing and balance (vestibular), smell (olfactory), facial sensation (trigeminal) and the facial nerve for expression, sensation of taste and closing of eyelids (Siacca et al. 2019). Injury or destruction of the cerebrum or the cerebellum can cause the patient to live a vegetative state whereas injury to the brain stem can cause brain death and this is due to its association with the heart and other organs. According to contemporary scholars such as Nadwi (2012), if the cerebrum has died and the doctors have confirmed that the brain is dead, then it is permissible to remove the life support even if his or her heart is functioning. Many of the fuqaha (jurists) are in agreement of this. However, concerning the death of the brainstem, there is a difference in opinion amongst contemporary scholars on whether it is considered the end of human life. The heart should not stop beating for the individual to be deemed dead. This was stated in the Islamic Fiqh Council Conference in 1986 in Amman. From the Shariah, it is thought that a person is dead if the following two signs develop: the heartbeat and breathing are ceased, and doctors confirm cessation cannot be reversed. Secondly, the brain function is ceased completely, and this has been confirmed by three neurologists, that the cessation cannot be reversed and the brain is disintegrated (Ghuddah, 1997). The respected scholars have utilised the people of the Cave as an example of how a loss of sensation and consciousness is insufficient to suggest that one is dead as Allah (The Most High) stated in the following verses: “So We cast [a cover of sleep] over their ears within the cave for several years. [Quran, Surah al-Kahf 18:11] Amongst the respected scholars is Al-Shawkani who explained in his book Fath Al-Qadeer about the above Quranic verse that the ears are shut with sleep to prevent them from hearing sounds (Phillips, 2004). His exegesis is based on Al – Mathoor is otherwise known as Al – Riwayah (Gnomic) and Al-Raei are also known as Al-Dirayah (Opinion) to provide this sound reasoning. Other scholars, for instance, Al-Qurtubi informed that the ears are used as a metaphor to elaborate on the corruption of oversleeping and via the ears, sleep was halted (Phillips, 2004). The ‘number of years’ has been confirmed in the same Surah: “And they remained in their cave for three hundred years and exceeded by nine.” [Quran, Surah Al-Kahf, 18:25] Allah (The Most High) states in the following verse: Then We awakened them that We might show which of the two factions was most precise in calculating what [extent] they had remained in time.” [Quran, Surah al-Kahf 18:12] Al-Qurtubi (2013) (may Allah have mercy upon him) explained that Allah wanted to express His knowledge where he already knew which of the two groups was able to calculate the accurate time (Phillips, 2004). Another respected scholar, Al-Shanqiti (2001) (may Allah have mercy upon him) agrees with this and adds that He (Allah) wanted to clarify to people who amongst the two groups were correct about the length of time but, he did not explain anything about the two groups. Majority of the scholars in Tafseer (exegesis) agree that one group is the People of the Cave, whereas the other group of people were the people of the city in which the youths lived. Other scholars agree that it was about the people who are amongst the believers and those who are amongst the disbelievers (Phillips, 2004). The difference in opinion further highlights the wisdom of the Almighty (The Most High) where one would question and also in how resurrection is real and where we will all be resurrected and; Allah (The Most High) can do all things. It was a test for the youths as they were unaware of how long they had slept. Allah (The Most High) answered their prayers and kept those people away whilst they slept in the cave. It is also a reminder of how we should put trust in Allah (The Most High) every time a trial rises. The state of the youth is concluded in the following verse: “And you would have thought them awake while they were asleep and I turned them on their right sides and their left sides and their dog lay with its front legs stretched out at the entrance of the cave. Had you seen them you would have turned and fled filled with fear of them.” [Quran, Surah al-Kahf 18:18]. This suggests that when the People of the Cave woke up, it was not typically as that of the youth who sleep and wake up relaxed. Some of the scholars suggested that their appearance of being awake was concerning their eyes were open when asleep. Other scholars are in the opinion that they were frequently turning on their right and left sides and He (Allah) did not mention the word ‘I’ because they turned as involuntary body movement. Furthermore, Prophet (peace be upon him) discouraged sleeping on the stomach (Phillips, 2004). There is a discrepancy in the number of times amongst the scholars of Tafseer where Abu Hurairah (may Allah have mercy upon him) mentioned twice a year, others mentioned once a year, Mujahid added it was due every seven years (Al-Qurtubi, 2013; Phillips, 2004; Al-Shanqiti, 2001). The outer brain The brain is surrounded by a bony skull (cranium) whose function is to protect the brain. There are also facial bones. The meninges is situated between the cranium and the brain and is one of the three tissue layers that protect the brain and spinal cord. The innermost layer of the meninges is the pia mater, the middle layer is the arachnoid and the outermost layer being the dura mater respectively. The subdural space divides the dura and arachnoid membrane whereas the subarachnoid space divides the arachnoid and pia and this is where the cerebrospinal fluid flows. In addition, the major arteries of the brain and the arachnoid trabeculae flow in the subarachnoid space. The arachnoid trabeculae are strands of arachnoid mater connective tissue. The epidural space exists between the calvarium in the roof of the skull and the superior surface of the dura (Rea, 2015; Ghannam and Al Kharazei, 2020). The pia mater consists of collagen, reticular fibres and many blood vessels that deepen into the surface of the brain (Rea, 2015). The collagen fibres form bundles outside the reticular tissue that surrounds the spinal cord (Rea, 2015). The outer layer of the pia is the epipial and comprises of collagen fibres whereas; the intima pia layer consists of elastic and reticular fibres (Ghannam and Al Kharazei, 2020). Arachnoid is a delicate, thin, avascular elastic membrane and consists of blood vessels that vary in size. It is situated between the dura and pia mata. The primary function of the arachnoid is involved in the cerebrospinal fluid via the subarachnoid space (Rea, 2015; Ghannam and Al Kharazei, 2020). The dura mater comprises of a bi-layered white non-elastic membrane where the outer layer is known as the periosteum. It comprises of osteoblasts and fibroblasts to give strength to the dura. The meningeal layer is close to the brain tissue. Both layers fuse to form two dural reflections and venous sinuses. The dural reflections consist of two special folds: the tentorium cerebelli and falx cerebri (Rea, 2015). The falx is sickle-shaped and divides the right and left of the cerebral hemispheres whereas the tentorium divides the upper and lower area of the brain where it predominantly runs between the cerebellum and occipital lobes (Rea, 2015). The cerebrospinal fluid (CSF) is a clear fluid in channels that provides support to the brain and spinal cord. The CSF produced in these channels are called ventricles in the choroid plexus; the CSF passes through the subarachnoid via the foramina of Luschka (Rea, 2015). The brain maintains the balance in the production and absorption of the CSF. There are four ventricles in the ventricular system: two lateral ventricles are situated in the cerebral hemispheres that communicate with the third ventricle (thalamus and hypothalamus) via the Foramen of Munro. The third ventricle is situated in the centre of the brain and communicates with the fourth ventricle via the Aqueduct of Sylvius (Rea, 2015). The hypothalamus is a small structure consisting of grey matter and regularly communicates with the pituitary gland to maintain homeostasis. The anterior hypothalamus and preoptic area comprise of temperature-sensitive neurons that respond to fluctuations of the internal temperatures by initiating thermoregulatory responses required to restore a constant temperature (Molitch, 2012). To lower heat production, cutaneous vasodilation, sweating and; panting occurs whereas to elevate the body heat, cutaneous vasoconstriction, shivering and; the production of metabolic heat production occurs (Molitch, 2012). The hypothalamic control is required for several hormonal secretions: vasopressin, oxytocin, thyroid-stimulating hormone (TSH), follicle-stimulating hormone (FSH), adrenocorticotropic hormone (ACTH) and leutinizing hormone (LH). It is also involved in the control of sleep where there are specialised hormones situated in the rostral and caudal area of the hypothalamus responsible for this. This highlights the importance of the hypothalamus in the sleep-wake cycle (Henning, 2001; Card and Rinaman, 2002, Puelles et al. 2012). The hypothalamus also forms part of the emotional Limbic System where it is at the centre with access to various neural pathways. The function of the limbic system is in various types of emotions from positivity (love, joy and confidence) and negativity (sad, anger and anxiety) as well as memory (Adnan, 2012). Besides the hypothalamus, the emotional limbic system also consists of the hippocampus, limbic cortex, septal area, amygdala and the subicular complex (Rajmohan and Mohandas, 2007). The hippocampus is a trilaminate structure that is ca. 5cm in size and consists of the outer, middle pyramidal and inner polymorphic layer (Rajmohan and Mohandas, 2007). The amygdala is an almond-shaped structure within the temporal lobe and consists of various forms of nuclei: basolateral, cortical-like, centromedial, amygdaloid and extended amygdala. The limbic cortex is composed of the cingulate and parahippocampal gyri and extends from the anterior of the amygdala to the splenium of the corpus callosum which comprises of the dentate gyrus, hippocampus and subicular complex (Rajmohan and Mohandas, 2007). The septal area consists of grey matter and, the structure of the limbic system collectively is adapted to perform its function as mentioned in the Quran in verse 25:2.  Figure 2: An MRI scan of the brain (Rasuli and Elgendy, 2020) Overall, the brain is a complexed structure and; its anatomy and functional organization allow us to sense, question and respond to matter through behaviour and language or speech. The cerebral cortex primarily plays a key role in this from emotion to cognition, movement and memory and; this is coordinated with the cerebellar cortex. Next month, we will discuss the cardio physiology of the heart and what the Glorious Quran states about it. The human body is filled with signs and greatness of Allah's creativity by the ability to know and understand what is wrong from what is right with a clear mindset that ignites peace, love, harmony amongst humanity and I end this section with the following verse from the Quran where Allah (The Most High) states: So which of the favours of your Lord would you deny? [Quran, Surah Al Rahman, 55: 37-38] References
Adnan, A. (2012) The Uniqueness Of The Brain Creation. Available online: https://knowingallah.com/en/articles/the-uniqueness-of-the-brain-creation/ Al-Qurtubi, M.A. (2013) Al-Jami‘ li Ahkam al-Qur’an, 9 – 10. Beirut: Risalah Publishing Al-Shanqiti, M. A (2001) Adwaa Al-Bayaan, 4. Beirut: Dar ibn Hazm. Al-Shawkani, M.A. (1994) Fath Al-Qadir, 5, Beirut: Dar Al-Fikr. Baum, G., Cui, Z., Roalf, D., Ciric, R., Betzel, R., Larsen, B., Cieslak, M., Cook, P., Xia, C., Moore, T., Ruparel, K., Oathes, D., Alexander-Bloch, A., Shinohara, R., Raznahan, A., Gur, R., Gur, R., Bassett, D. and Satterthwaite, T., (2019) Development of structure–function coupling in human brain networks during youth. Proceedings of the National Academy of Sciences, 117(1), pp.771-778. Bonner, K., Borlay, D., Kutten, O. and Quick, Q., (2020) Inhibition of the Spectraplakin Protein Microtubule Actin Crosslinking Factor 1 Sensitizes Glioblastomas to Radiation. Brain Tumor Research and Treatment, 8(1), p.43. Boudreau, C., Yang, I. and Liau, L., 2005. Gliomas: advances in molecular analysis and characterization. Surgical Neurology, 64(4), pp.286-294. Cancer Research UK (2020) ‘What are Brain Tumours?’ Available online: https://www.cancerresearchuk.org/about-cancer/brain-tumours/about Card, J. and Rinaman, L., (2002) Hypothalamus. Encyclopedia of the Human Brain, pp.525-535. Chouinard, P. and Paus, T., (2006) The Primary Motor and Premotor Areas of the Human Cerebral Cortex. The Neuroscientist, 12(2), pp.143-152. Clark, R., (2017) Current Topics Regarding the Function of the Medial Temporal Lobe Memory System. Behavioral Neuroscience of Learning and Memory, pp.13-42. Collins, A. and Koechlin, E., (2012) Reasoning, Learning, and Creativity: Frontal Lobe Function and Human Decision-Making. PLoS Biology, 10(3), p.e1001293. Flinker, A., Korzeniewska, A., Shestyuk, A., Franaszczuk, P., Dronkers, N., Knight, R. and Crone, N., 2015. Redefining the role of Broca’s area in speech. Proceedings of the National Academy of Sciences, 112(9), pp.2871-2875. Ghannam, J. and Al Kharazi, K. (2020) Neuroanatomy, Cranial Meninges. Available online: https://www.ncbi.nlm.nih.gov/books/NBK539882/#_NBK539882_pubdet_ Ghuddah, A. (1997) Qararat wa-Tawsiyat Majma' al-Fiqh al-Islami. Damascus: Dar Al-Qalam. Gilbert‐Jaramillo, J., Garcez, P., James, W., Molnár, Z. and Clarke, K., (2019) The potential contribution of impaired brain glucose metabolism to congenital Zika syndrome. Journal of Anatomy, 235(3), pp.468-480. Gray, H., Warwick, R. and Williams, P. (1980) Gray’s Anatomy UK: Churchill Livingstone. Guell, X., Schmahmann, J., Gabrieli, J. and Ghosh, S., (2018) Functional gradients of the cerebellum. eLife, 7. Hennig, J., (2001) Hypothalamus. International Encyclopedia of the Social & Behavioral Sciences, pp.7113-7118. Hoffmann, M. (2019) Picture of the brain. Available online: https://www.webmd.com/brain/picture-of-the-brain#1 Islamic Fiqh Council (1986) Organisation of the Islamic Conference. Jordan: Amman. Jawabri, K. and Sharma, S. (2020) Physiology, Cerebral Cortex Functions. Available online: https://www.ncbi.nlm.nih.gov/books/NBK538496/#_NBK538496_pubdet_ Kiernan, J., (2012) Anatomy of the Temporal Lobe. Epilepsy Research and Treatment, 2012, pp.1-12. Lapointe, S., Perry, A. and Butowski, N., (2018) Primary brain tumours in adults. The Lancet, 392(10145), pp.432-446. Margulies, D., Ghosh, S., Goulas, A., Falkiewicz, M., Huntenburg, J., Langs, G., Bezgin, G., Eickhoff, S., Castellanos, F., Petrides, M., Jefferies, E. and Smallwood, J., (2016) Situating the default-mode network along a principal gradient of macroscale cortical organization. Proceedings of the National Academy of Sciences, 113(44), pp.12574-12579. Marshall, J. and Morriss-Kay, G., (2004) Functional anatomy of the human brain. Journal of Anatomy, 205(6), pp.415-415. McKinney, P.A., (2004) Brain tumours: incidence, survival, and aetiology. Journal of Neurology, Neurosurgery & Psychiatry 75:ii12-ii17. Minniti, G., Filippi, A., Osti, M. and Ricardi, U., (2017) Radiation therapy for older patients with brain tumors. Radiation Oncology, 12(101). Molitch, M., (2012) Neuroendocrinology and the Neuroendocrine System. Goldman's Cecil Medicine, pp.1425-1431. Molnár, Z., Clowry, G., Šestan, N., Alzu'bi, A., Bakken, T., Hevner, R., Hüppi, P., Kostović, I., Rakic, P., Anton, E., Edwards, D., Garcez, P., Hoerder‐Suabedissen, A. and Kriegstein, A., (2019) New insights into the development of the human cerebral cortex. Journal of Anatomy, 235(3), pp.432-451. Nadwi, M., Thackray, S. and Ahmed, S. (2012) Al-Fiqh Al-Islami: According to the Hanafi Madhhab: Zakah, Fasting and Hajj Volume 2 UK: Angelwing Media. Neulinger, K., Oram, J., Tinson, H., O’Gorman, J. and Shum, D., (2015) Prospective memory and frontal lobe function. Aging, Neuropsychology, and Cognition, 23(2), pp.171-183. Nourski, K., (2017) Auditory processing in the human cortex: An intracranial electrophysiology perspective. Laryngoscope Investigative Otolaryngology, 2(4), pp.147-156. Phillips, A.B. (2004) Tafseer Soorah Al-Kahf Qatar: IOU University Press. RajMohan, V. and Mohandas, E., (2007) The limbic system. Indian Journal of Psychiatry, 49(2), p.132. Rasuli, B. and Elgendy, A. (2020) Limbic system. Available online: https://radiopaedia.org/articles/limbic-system?lang=us Rea, P., (2015) Essential Anatomy and Function of the Spinal Cord. Essential Clinical Anatomy of the Nervous System, pp.121-131. Sciacca, S., Lynch, J., Davagnanam, I. and Barker, R., (2019) Midbrain, Pons, and Medulla: Anatomy and Syndromes. RadioGraphics, 39(4), pp.1110-1125. Singh, R. (2020) Cerebellum: Its Anatomy, Functions and Diseases https://www.intechopen.com/online-first/cerebellum-its-anatomy-functions-and-diseases Watson, C., Paxinos, G. and Puelles, L. (2012) The Mouse Nervous System. Available online: https://www.sciencedirect.com/book/9780123694973/the-mouse-nervous-system#book-info Yang, Y., Raine, A., Narr, K., Lencz, T., LaCasse, L., Colletti, P. and Toga, A., (2007) Localisation of increased prefrontal white matter in pathological liars. British Journal of Psychiatry, 190(2), pp.174-175.  My journey in understanding how the anatomy and physiology of the human body with the Glorious Quran interconnects continues. This is associated with Tawassum (ability to understand) where I am inspired to observe and reflect on nature which provides us with a meaningful purpose and spiritual nourishment. Allah (The Most High) says: “Indeed in that are signs for those who discern.” [Quran, Surah Al Hijr, 15:75] The ability for us to reflect and analyse is known as Tadabbur and is derived from ‘dabara' or ‘dubr' meaning back (Chaudhary, 2020). When we observe the face of someone, we do not look at their back nor effort that is deepened. Thus, if we want to understand the Glorious Quran, we need to deepen our exploration of divine speech of Allah (The Most High) (Chaudhary, 2020). Therefore, there is a potential benefit through Taffakur (thinking) and Taddabur (reflection) that function in an integrated matter. Allah (The Most High) states: “Do they not reflect on the Qur’an carefully (yatadabbarun al-Qur’an)?” [Quran, Surah an-Nisa’, 4:82] In another verse, Allah (The Most High) states: “We created man of the best stature (mould)” [Quran, Surah At-Tin, 95:4]. Allah (The Most High) has created humankind in the best form and amongst the anatomical details found in the Glorious Quran is the human senses that gives us the power to perceive the world around us. However, it must be emphasized that is the All-Powerful and He alone is in control of all things. Allah states in the Quran: "It is Allah who has created seven heavens and of the earth, the like of them. [His] command descends among them so you may know that Allah is over all things competent and that Allah has encompassed all things in knowledge." [Quran, Surah Talaq, 65:12] Human senses can be divided into internal and external senses that collaborate to assist with our health and well-being (Sempo et al. 2017). Internal senses are associated with feelings and emotion, for instance, happiness, gratefulness, sadness and anger. Thus, our internal senses are associated with our psychology on three levels: sub-personal, behavioural and phenomenal (Fulkerson, 2014). On the other hand, external senses are linked to the sensory system that consists of special sense organs that detect excitatory information from the environment (Knight, 2017). This is then relayed to the brain in the central nervous system to process into sensations via neural pathways (Gadhvi and Waseem, 2020). Our body contains a five-sense device, eyes to provide us with vision, olfaction via our nose, the ability to hear with our ears, taste (gustation) with our mouths, touch (tactile perception) with our hands and somatic sensation (Ibn Sina, 1952a; Sempo et al. 2017; Knight, 2017). Thus, the anatomy and physiology of the human senses are vital in understanding the different sensations (Gadhvi and Waseem, 2020). Dysfunctional effects of these modalities would decrease our ability to communicate and understand the world around us and; the diminished acuity will increase as we age (Knight, 2017). One of the dysfunction effects of the sensory system is cancer where there are side-effects of patients undertaking radiotherapy and chemotherapy (McWilliams, 2008). Patients with cancer lose their ability to taste and smell due to the cancer therapies administered that can dysfunction the olfactory and taste receptor cells causing morphological changes and dysgeusia ( slight change in taste) to complete change in taste (aguesia) for sweet, sours, bitter and umami food flavouring and can also affect the peripheral system (Altundag and Cayonu, 2016, McWilliams, 2008). Statistics have shown that there is a ca. 77% chance cancer patients have this symptom of an infrequent smell and is common amongst patients with head and neck cancer (Altundag and Cayonu, 2016). Besides, metabolic changes can also occur. Other diseases in response to dysfunctional effects of the sensory system include fungal infections, for instance, dry mouth, ulcers, thrush (Schiffman, 2007). Deficiencies, for instance, Vitamin A, niacin is associated with cancer (Rehwaldt et al. 2009) Allah (The Most High) states: “And Allah has extracted you from the wombs of your mothers not knowing a thing, and He made for you hearing and vision and intellect that perhaps you would be grateful” [Quran, Surah Nahl, 16:78] Furthermore, Al-Nahlawi (1983) informed that the heart has other functions besides pumping oxygenated blood around the body to provide nutrients for cells, tissues and organs. The heart provides thoughts, for instance, happiness and gratefulness and the ability to observe and visualise the development of science via assessment and results. This suggests that the human senses are fundamental in creating environmental sustainability and is embedded in the Quran and Sunnah and protected by the Maqaseed Al Shariah otherwise known as ‘The Objectives of Islamic Law' (Asmawati et al. 2020). There are two forms of Tafsir: Tafsir Al Maatoor (Traditional explanation) and Tafsir bil Al ra'yi (explanation with reason) and this can be achieved with our senses that have a vital function to shape our knowledge, understanding and contribution (Abbas, 1973; Asmawati et al. 2020). Ibn Qayyim (2018) mentioned that our human senses are blessings and will testify against us on the Day of Judgement where Allah has stated in the following verses: “This Day, We shall seal up their mouths, and their hands will speak to Us, and their legs will bear witness to what they used to earn.” [Quran, Surah Ya-Sin, 36:65] “On the Day when their tongues, their hands, and their legs or feet will bear witness against them as to what they used to do. [Quran, Surah An-Nur, 24:24]. This emphasises how our human senses correlate with our faith where we listen to the Fardh (mandatory) and the Sunnah and avoid what is prohibited (Ibn Qayyim, 1991). For instance, we listen to the Quran, a lecture or a halaqa and avoid things that affect the heart and idle speech. The process of how our human senses function Our body consists of specialised cells called receptors that receive the stimuli and translate it into signals. There are various forms of receptors summarised in Table 1. Examples of the somatovisceral receptors include mechanoreceptors for touch, thermoreception due to the alteration of the hot and cold weather and pain (nociception) to regulate homeostasis, blood pressure and respiratory rate (Gebhart, 1995). Table 1: The various types of receptors 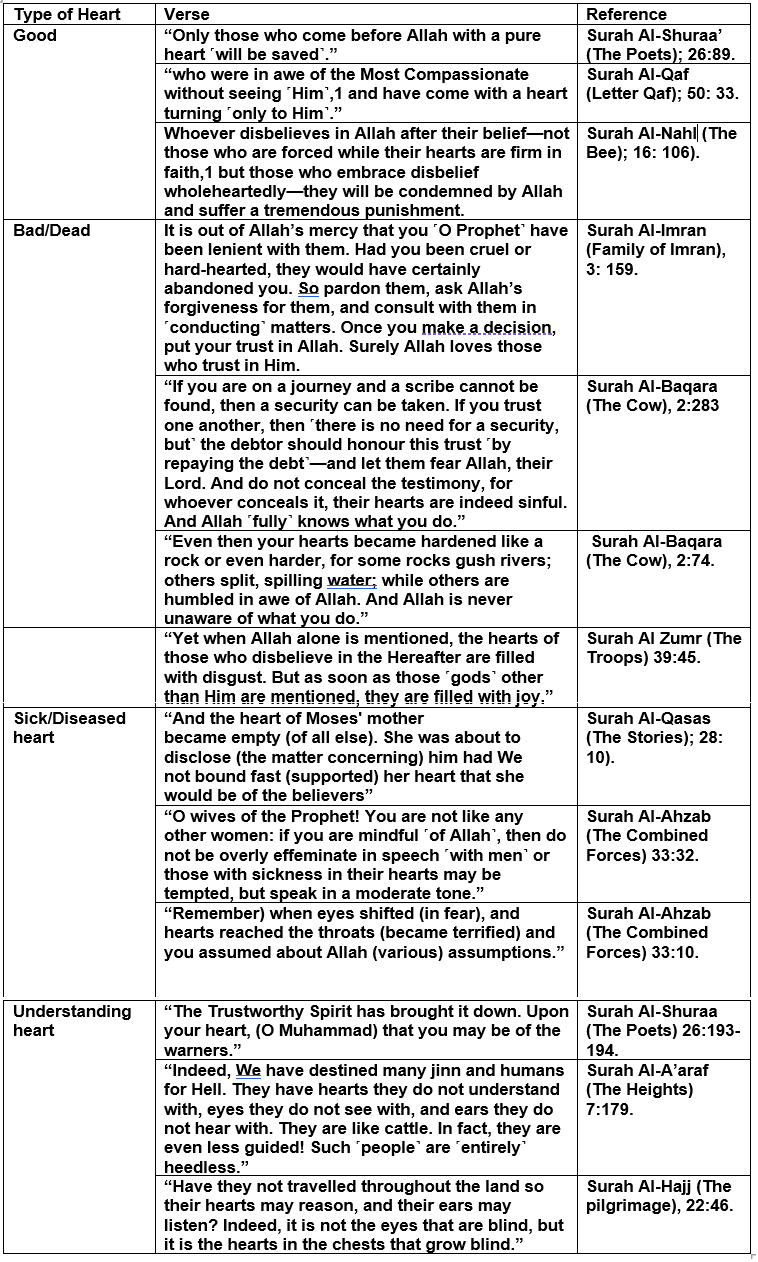 There are three types of nerves otherwise, known as neurones presented in Figure 1. Their structures vary but they all have dendrites to receive signals and connect with the cell body. Axon facilitates action potential (Catala and Kubris, 2010). The myelin sheath insulates the axon and, the axon terminal connects neurons via a synaptic transmission (Allen and Schwartz, 1940).  Figure 1: The three types of neurons The signal is transmitted as action potential via the sensory neuron from the dorsal ganglion root in the peripheral nervous system where it is then converted to electrochemical energy in the sensory cortex in the spinal cord (Allen and Schwartz, 1940). The central nervous system consists of the brain and spinal cord. This is known as transduction. The sensory neuron is of a pseudounipolar sub-type where it has no dendrites. The peripheral branch extends from the cell body to the skin, joints and muscles, whereas, the central branch extends from the cell body to the spinal cord (van Stralen and Dijikerman, 2017). There are two pathways in how sensory neurons transmits the nerve impulses to the spinal cord that conveys somatosensory input as illustrated in Figure 2. Spinothalamic pathway comprises of pain, touch, temperature and sensations to several thalamic nuclei (Allen and Schwartz, 1940; Irvine and Clark, 2017; van Stralen and Dijikerman, 2017). The second pathway is the dorsal column which is required for touch, vibrations and proprioception (Ghanty and Schragg, 2019). 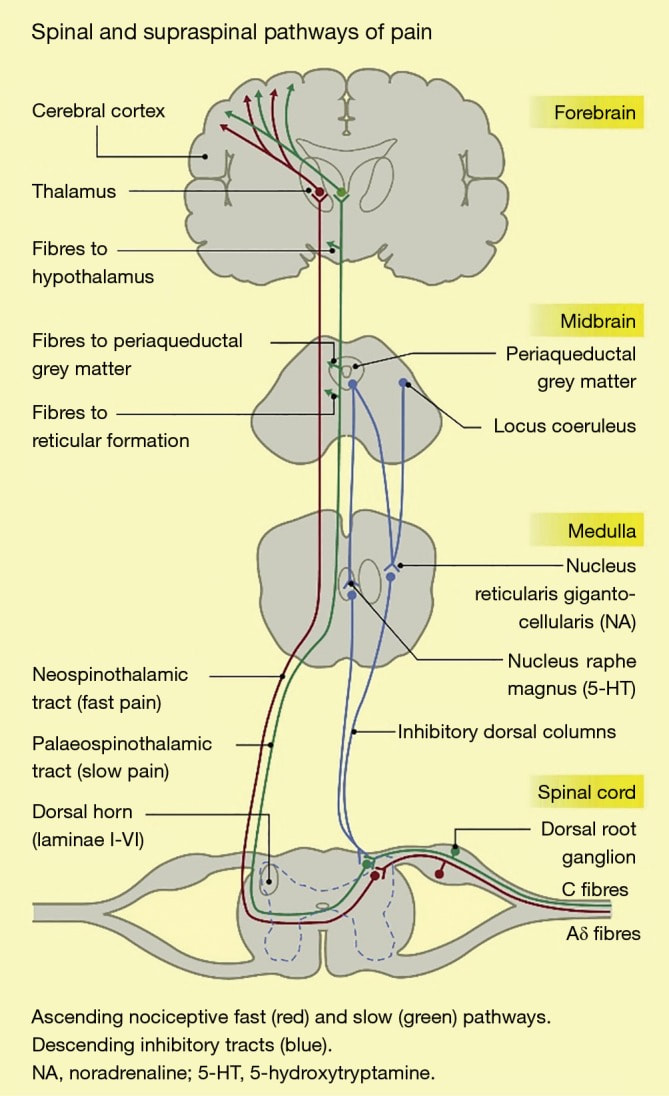 Figure 2: The neural pathways: supraspinal and dorsal column (Ghanty and Schraag, 2019) For example, for hearing to occur, the hair cells of the auditory system act as receptor cells cause the stereocilia to bend. There is an energy transfer from mechanical energy to electrochemical energy in response to the flow of ions via channels into the membrane to generate cell membrane potentials which could be depolarization or excitation (Hudspeth and Gillespie, 1994). The intensity of the potential depends on the time, rate and strength of the stimulus. There is a constant force in the bending of the stereocilia. The mechanical mechanism is stimulated by the proteins actin and myosin to reset the tension and transduction to the resting state where the sensory cell can respond to new stimuli (Hudspeth and Gillespie, 1994; Sokolowski 2007). Upon the signal reaching the central nervous system, the relay neurons allow the sensory neurones and motor neurons to communicate (Bishop, 1980). The fibres are classified based upon sensation, size of diameter and velocity (Catala and Kubris, 1980). The classification is known as Erlanger Gasser and consists of four groups: Group 1 alpha are fibres from the primary endings of muscle spindles. Group 1 beta is from Golgi tendons. Group 2 beta is from secondary endings of muscle spindles as well as touch receptors in the skin. Group 3 delta is from muscle endings and skin. Group 4 are from the skin and muscles (Dubin and Patapoutian, 2010). The motor neurones function in controlling muscle movements where it releases neurotransmitters that associate with the receptors in muscles (Catala and Kubris, 2010). Therefore, the sensory system and the central nervous system is vital to interconnect to produce a response. The power of hearing Hearing is one of the human senses that has been created by Allah (The Most High) before vision in the foetus where he or she can hear the voice of the mother whilst it is in the womb. We have been blessed with a pair of ears to function in hearing, listening, communication, balance, consciousness and alertness. The Glorious Quran has various evidence of its physiological purpose. “We created man from a fertilizing sperm, to test him; and We made him hearing and seeing” [Quran, Surah Insaan, 76:2] "Why are its verses not explained in detail [in our language]? Is it a foreign [recitation] and an Arab [messenger]?" Say, "It is, for those who believe, a guidance and cure." And those who do not believe - in their ears is deafness, and it is upon them blindness. Those are being called from a distant place.” [Quran, Surah Fussilat, 41:44] “ It is He who produced for you the hearing, and the eyesight, and the feelings. But little gratitude you show “And if We had made it a non-Arabic Qur'an, they would have said” [Quran, Surah Muminoon, 23:78] “Do they have feet by which they walk? Or do they have hands by which they strike? Or do they have eyes by which they see? Or do they have ears by which they hear? Say, [O Muhammad], “Call your ‘partners’ and then conspire against me and give me no respite.” [Quran, Surah Haqqah, 69:12] The ear is divided into the outer, middle and inner ear as presented in Figure 3. The ears alter the vibrations perceived as sound where the outer ear consists of the pinna and the external auditory ear canal. The pinna is made of cartilage and gains high-frequency sound waves where they are funneled down the ear canal that acts as a resonating tube and protective barrier to the tympanic membrane. The ear canal consists of the sweat gland and oily sebaceous glands that together form earwax (Alper et al. 2017). The tympanic membrane is also known as the eardrum is a thin membrane that associates with the Eustachian and mastoid air cells (Alper et al. 2017). It forms part of human auditory apparatus (Alper et al. 2017). A perforated eardrum can cause hearing loss (Mayo clinic, 2020). This is why Allah says in the Quran: "Among them are those who listen to you; but We place covers over their hearts, to prevent them from understanding it, and tear in their ears. Even if they see every sign, they will not believe in it. Until, when they come to you, to argue with you, those who disbelieve will say."This is not but legends of the former peoples." [Quran, Surah Al-Anaam 6:25] The middle ear is where mechanical vibrations can be heard in the membrane. Most sounds are transmitted by air to cause vibration, however poor vibration occurs where two areas differ in the density and speed of sound such as water. The eustachian tube (pharyngotympanic tube) ensures the pressure in the middle ear is balanced with the pressure in the atmosphere. The vestibular complex in the inner ear also facilitates and is based on receptors that sense equality. The middle ear extends from the air passages of the nose and sinus lining the respiratory membrane. It absorbs the gases, carbon dioxide and oxygen from the air in the middle of the ear and; this may produce pain. The back end of the nose in the nasopharynx consists of cartilage and muscle (Alper et al. 2017). The tympanic membrane transfers the mechanical vibrations to auditory ossicles. Auditory ossicles are three small bones found in the air cavity of the middle ear: malleus (hammer), incus (anvil) and stapes (stirrup) (Richardson et al. 1939). The stapes bone pushes the oval window in and out the vibrations to the spiral-shaped organ of Corti otherwise known as the cochlea. They transfer the vibrations to the inner ears (Alberti, 2005). The vibrations are transduced by the cochlea to the perilymph via the ossicular chain into a nerve impulse by the delicate hair cells that detect pressure in the fluid cavity where receptors are activated and; is carried along the statico-acoustic nerve/ vestibulocochlear nerve from the cochlea to be processed in the brain via the auditory pathways to produce sound (Alberti, 2005; Richardson et al. 1939). The nerve fibres split where they pass one side of the brain and; the rest remain unchanged because they ascend to the hindbrain to the midbrain and the cerebral cortex (Alberti, 2005). This highlights the auditory function of the ears and its role in balance. 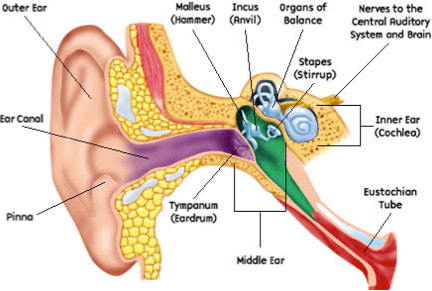 Figure 3: The structure of the ear (Shannon, 2010). The power of vision We initiate in the wombs of our mothers without vision and then blessed with the visual tool, our two eyes, following the development of the primitive features of our ears. The primary function of the eyes is to perceive the outside world where we can capture, adjust and transform the size, colour (stereopsis), type and length of the distance of what we see via neuroreceptors. This is based upon the light patterns where it can either reflect, refract, diffract, dilate or constrict (Zhu et al. 2012). “And Allah has extracted you from the wombs of your mothers not knowing a thing, and He made for you hearing and vision and intellect that perhaps you would be grateful” [Quran, Surah Nahl, 16:78] To be able to thank Allah (The Most High) for this blessing would be insufficient. Allah is Our Inventor. Our Creator. Our eyes are also the door to the aperture of our hearts; hence it contains vivid information of our emotions and well-being. It allows us to be aware of trials and become more conscious. Ibn Al-Qayyim (1991) stated: “Contained within the crystal is a lamp, and it is the light which is in the wick – and it is its carrier, and for that light, there is an ingredient – and it is oil which has been pressed out of an olive that originates from the most equitable of places. The sun gleams upon it at the first portion of the day as well as its latter; hence its oil is from the clearest of oils and the furthest of them from cloudiness, such that due to its clarity it virtually illuminates without flame – this is the ingredient of the light of the lamp. Likewise is the ingredient of the light of the lamp which is in the heart of the believer, it is derived from the tree of revelation which is from the greatest of factors for blessing – and the furthest of them from misguidance.” Allah (The Most High) states: “So have they not travelled through the earth and have hearts by which to reason and ears by which to hear? For indeed, it is not eyes that are blinded, but blinded are the hearts which are within the breasts.” [Quran, Surah Al-Haj, 22:46] This highlights the importance of our heart and its natural connection with the eyes from a spiritual and physical context. From the spiritual perspective, Allah looks into the quality of our hearts whereby intention, knowledge, belief and relationship are key factors to determine the viability of the heart, for if the stated elements are sound, the heart will not be diseased. On the other hand, our eyes also reveal pathological features that relate to our heart. Tiny, blood vessels in the eyes called the retinal vasculature associate with the heart. High blood pressure or hypertension can cause visual damage due to the significant pressure within the blood vessels. This can lead to blurry vision, blood clots and bleeding in the eyes. Besides, it can also lead to strokes hence why an eye examination takes place to investigate the presence of constriction to blood vessels, spots and swelling. The anatomical features of our eyes The human eye has three layers: outer, middle and inner layers as presented in Figure 4. The outer layer consists of the sclera and cornea. The middle layer comprises of the choroid, iris and the ciliary body. The inner layer contains the retina. The distinctive features of the eye together allow the focusing of the images on the retina to exert their regulatory functions of the light, protection, motion and provide nutrition. The complexity of the eyes and the nerve fibres that associate the eyes with the central nervous system cannot be transplanted nor reconstructed. This further highlights the extent of the engineering skills that Allah (The Most High) possess. For He is All-Seeing. All-Aware, The inventor and the Creator. “Vision comprehends Him not, but He comprehends (all) vision. He is the Subtle, the Aware. Insights have certainly come to you from your Sustainer; then whoever sights, does so for his own self, and whoever is blinded, does the same. And (say): I am not over you an overseer.” [Quran, Surah Al Anaam, 6:103-104] 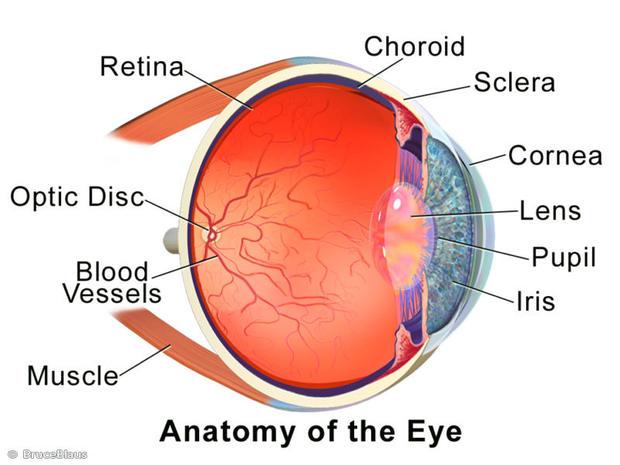 Figure 4 The structure of the eye (Blaus, 2020) Amongst the features in the outer layer is the cornea, a clear, transparent and dense layer with a horizontal and vertical diameter, 11.5 mm and 10.5 mm respectively (Muller et al., 2003; Farjo et al., 2009). It refracts and transmits light to the pupil, lens and retina (Muller et al. 2003). It also protects the eyes from trauma, damage and infection (Van Burskirk, 1989). Most of the corneal nerves are sensory nerves derived from the ophthalmic branch of the trigeminal nerve (Muller et al. 2003; Farjo et al. , 2009). The cornea is situated in the anterior area of the fibrous tunic which is presented in front of the iris and pupil and consists of four distinctive sub-layers: Corneal epithelium, Bowman's membrane, Corneal stroma, Descemet's membrane and Corneal endothelium (Van Buskirk, 1989). The Corneal epithelium has an impermeable and stable basement membrane comprising of several layers of wing cells and one basal cell layer due to the cell junctions (McCaa, 1982). The Bowman's membrane is a clear and homogenous layer. The collagenous feature of the corneal stroma maintains the mechanical strength, structural integrity and diptropic stability of the cornea and forms 90% of the cornea (Van Burskirk, 1989). The stromal keratocytes secrete the collagen and proteoglycans. Proteoglycans regulate the hydration level where the fluid flux from the stroma produces water required for transparency; deturgence (McCaa, 1982; Muller et al. 2003). The Descemet's membrane is a strong, homogeneous basement membrane. It consists of endothelial cells that provide an elastic feature and; this thickens with age where the anterior end is banded and; the posterior ending is amorphous (Zhu et al. 2012). The Corneal endothelium has a single cell layer containing flat, cuboidal cells that maintain the dehydration of the corneal tissue. Destruction to the structure of the endothelium can cause swelling and loss of transparency of the cornea (McCaa, 1982). The sclera is a white, opaque connective tissue situated in the posterior end of the tunic (Willoughby et al. 2010). Its function is to maintain the shape of the eye and protect the internal structures from damage. It is covered by a transparent, mucous membrane called the conjunctiva (McCaa, 1982). The iris is the coloured area of the eye situated in the middle ocular layer. It acts as a window shutter or a diaphragm where it has an involuntary control in the size of the pupil and the amount of light that enters the retina (McCaa, 1982). The autonomic nervous system consists of the sympathetic and parasympathetic nervous system. The sympathetic system has a fight or flight response where it responds to fear, bright light causing the radially oriented pupillary dilator muscle to contract in the iris which results in the dilation of the pupil (mydriasis). Similarly, the nervous system responds dramatically when the astronauts travel to space. Amongst the symptoms felt is dizziness and nausea during the initial days and; this progresses to the blurred vision that corresponds to symptoms when drunk. Allah (The Most High) says: “And [even] if We opened to them a gate from the heaven and they continued therein to ascend, They would say, "Our eyes have only been dazzled. Rather, we are people affected by magic." [Quran, Surah Al Hijr, 15, 14-15] The parasympathetic nervous system has a rest or digest response where it conserves energy for sleep, digestion and seeing during dim light where the pupil constricts (miosis). The scholars such as Ibn Amir Al-Hajj (May Allah have mercy upon him) states: “Sleep is a state that occurs to the intellect that necessitates the incapacity of a person to perceive sensory things, to conduct involuntary actions, and the general use of the intellect.” (Dar Al Ifta, 2020). Another feature found in the middle layer is the uvea. The uvea provides nutrients where the posterior end is the choroid and; the other area of the uvea is called the ciliary body (Schubert, 2009). The choroid is a vascular layer that consists of blood vessels that provide oxygen and nutrients to the outer retinal layers. On the other hand, the ciliary body produces intraocular fluid known as the aqueous humour. Additional roles of the ciliary body are to provide muscle support, control the shape and power of the lens (McCaa, 1982). The lens is situated behind the iris and is supported by a suspensory ligament; the zonule (McCaa, 1982). Behind the lens is a vitreous gel that occurs between lens and retina (McCaa, 1982). The retina is situated in the inner layer surrounding by the dura mater; a dense fibrous tissue. It is a complex, delicate membrane of neurones and is protected by the sclera and cornea (Schubert, 2009; Masland, 1986). There are various types of neurones present in the retina: bipolar, photoreceptors, amacrine, ganglion cells, horizontal cell and Mullerian glia. The photoreceptor, bipolar, horizontal, amacrine and ganglion process whereas the glial cells organise the back of the retina (McCaa, 1982). There are two types of photoreceptor cells: rods and cones. The cones translate light into colours and vision and have pigments with a high absorption peak in the blue and green spectrum (McCaa, 1982). The rods translate the light into peripheral vision and motion and have low light levels (McCaa, 1982). However, this is dependent on several factors, for instance, the wavelength, the intensity of the light and the area illuminated. The macula lutea in the retina comprises of xanthophylls pigment and several ganglion cells. Within the macula, the fovea has high levels of cones required for central vision; whereas the lower end of the fovea contains dense cones and is known as the foveola. The density of the foveola allows the synaptic terminals and the ganglion cells to the centre where Henle's fibres are formed between the nuclei and synaptic terminals (McCaa 1982). The retinal pigment epithelium (RPE) is arranged in a hexagonal format and; the pigment granules are found in the apical end of the RPE where lipofuscin and melanin are produced (McCaa, 1982). RPE consists of two blood-retinal barriers: retinal and the choroid where the former supplies the inner retina whereas; the latter received from the choroid circulation via diffusion. Additional roles of the RPE include pigment formation, adhesion, production of growth factors, wound healing and metabolism of Vitamin A (McCaa, 1982). The visual pathway - how can we see? The photoreceptor cells capture the image in the back of the retina. It is inverted as it progresses through the lens where there are two optic tracts. The left optic tract has half of the image projected onto the nasal retina of the right eye and the temporal retinal of the left eye. On the other hand, the right optic tract has a left image projected onto the temporal retinal of the right eye and the nasal retina of the left eye. This is processed and converted to nerve impulses or electrical signals (phototransduction). The signal passes from the axon of the ganglion to the optic disc and then the second cranial nerve called the optic nerve (Willoughby et al. 2010). The optic nerves from each eye produce the optic chiasm where the fibres from the nasal retina travel to contralateral optic tract; whereas the fibres from temporal retina remain ipsilateral (McCaa, 1982). The is presented in Figure 5. The optic tract travels to the specific cerebral hemisphere to the lateral geniculate nuclei (LGN). The LGN is situated in the thalamus and consists of neurons that send axons to the ipsilateral primary visual cortex via fibres radiation to process the sensory information. There are two types of optic radiation: the upper optic radiation transfers the fibres signal to the cortex via the parietal globe whereas the lower optic radiation achieves this via the temporal lobe and this is called Meyer's loop (Schubert, 2009; Masland, 1986). Upper optic radiation carries fibres signal to the parietal globe to reach the cortex. Lower optic radiation carries fibres via temporal lobe and; this is called Meyer's loop to reach the visual cortex. Once at the cortex, it will process sensory information (Schubert, 2009). The horizontal and amacrine cells modify and control signal. Allah says in the Quran: “Have We not made for him two eyes?” [Quran, Surah Balad, 90:8]  Figure 5: The visual pathway (Garrity, 2020) The power of smelling The function of the nose is to provide an exchange of the air between the environment internally and externally where oxygen is inhaled and; carbon dioxide is exhaled (Jones, 2001). The anatomical structure and function of the nose and paranasal sinuses are fundamental for olfaction, the modification and transformation of inspired air towards 38 oC and 100% relative humidity (Proctor and Adams, 2008; Guerkink, 1983). Inside the nose, there are two cavities: nasal cavity and paranasal in the centre of the face and are also found in the skull (Jones, 2001; Proctor and Adams, 2008; Sahin-Yilmaz and Naclerio, 2011). The left and right nasal cavity (choanae) is divided by a middle wall called a septum. The septum is composed of cartilage (anterior) and bone (posterior) that together aid in increasing the mucosal surface area (Sahin-Yilmaz and Naclerio, 2011). At the bottom of the nasal cavity, there is a floor which extends to the back where it associates with the nasopharynx. The nasopharynx is at the back of the throat and interconnects the nasal cavity with the oropharynx. On the side of the nasal wall are little projections called turbinates (conchae) as presented in Figure 6. They contain cancellous bone made with trabeculae surrounded by respiratory epithelium and function in increasing the mucosal surface between the range 100cm to 200 cm to filter and humidify the air (Sahin-Yilmaz and Naclerio, 2011). There are three types of turbinates: inferior (lower), middle, superior (upper) and sometimes a fourth one called supreme.  Figure 6: The anatomical features of the nose (Sabale et al. 2020) Sinuses produce mucus to moisturize the nasal cavity, humidify the air, lighten the weight of the head, protect the skull from damage and allows a resonating voice to occur (Thanc Foundation, 2020). There are four main types of sinuses: maxillary, ethmoid, frontal and sphenoid sinuses. Maxillary sinuses are found in the cheek and contain mucus to drain into the nasal cavity under the middle turbinate. This commonly where sinonasal cancer arises from. Ethmoid sinuses are composed of 10 to 20 small sinuses that have thin walls and; the mucus is extracted under the middle and superior turbinates (Sahin-Yilmaz and Naclerio, 2011). The frontal sinuses are situated in the forehead and drain the mucus from the nasal cavity below the middle turbinate to a passage called the nasofrontal duct. Sphenoid sinus resides at the base behind the nose below the superior turbinate. Besides, there is a tear duct that drains the tears from the eyes under the inferior turbinate (Sahin-Yilmaz and Naclerio, 2011). Allah states: “We will brand him upon the snout" [Quran, Surah Al Qalam, 68:15]. Outside the nose, various cartilages are supported by the septum, for instance, the lateral (alar) has two at the top and two at the bottom. The lower lateral consist of medial and lateral cruca. The small muscles: nasalis, deptessor septinasi, levator labii superioris alaquei asi lower the nasal resistance and dilate the nostrils (vestibule) (Dion et al. 1978). Vestibule consists of stratified epithelium. The anterior nasal glands secrete the serous mucus and; this is where sniffing occurs that causes the stimulation of secretions. Humans have various types of receptors where the neuron in the olfactory cleft situates in the nasal cavity near the olfactory bulb and fossa. Amongst them are thermoreceptors who upon stimulation cause a nasal resistance in the airway. However, during inspiration, the warm air decreases the nasal resistance where there is ca. 50-75% resistance from ambient air to the pulmonary alveoli whereas, in the cold air there is an increase in the nasal resistance where there is more time for gas exchange in the alveoli and the air is more turbulent. This causes the inspired air to interact with the nasal mucosa and warmed as it reaches the nasopharynx (Connel and Fregosi, 1993; Cauna 1982). Posterior to the vestibule is the nasal valve where the dilator naris muscle increases the surface area and airflow from 40 to 150 mm squared (Sahin-Yilmaz and Naclerio, 2011). Al-Qastallani writes: “Let him sniff water three times to expel harmful things after he blows it out from his nose, for it cleans the airways through which the Quran is recited.” [Irshad Al Sari] Upon smelling, the sense receptors associate with the chemicals present in the air in the olfactory cleft transmit the smell to the brain via the hair-like cilial structures in the epithelium in the upper nasal cavity (Sahin-Yilmaz and Naclerio, 2011). They travel to the olfactory bulb that contains neurone cell bodies that transmit the peripheral information along the cranial nerves. This transcends to the olfactory nerves to the olfactory cortex in the cerebral cortex of the brain (Sahin-Yilmaz and Naclerio, 2011). They will then process all information about the intensity, hedonics and memory of the odour. Therefore, this amazing structure that is situated between the eyes has a prominent function where it is an olfactory organ and also is a doorway to the respiratory tract where it can sustain 20 to 30 L of airflow per minute and; if a higher volume of air is needed, a combination between oral and nasal breathing occurs (Sahin-Yilmaz and Naclerio, 2011). The power of tasting The oral cavity or the mouth is the space that initiates from the upper lip to the hard palate and consists of teeth, mandible, hard palate, buccal and gingival mucosa, floor, tongue and the circumvallate papilla as presented in Figure 7 (Cohen, 2013). The mouth has a gustatory sense for various tastes of what we consume by the presence of buds. In total, there are ca. 2,000 to 4,000 taste buds where the majority of buds reside on the tongue, the remainder can be found in the nasal cavity, oesophagus, epiglottis and the back of the throat (InformedHealth.org, 2016). Allah (The Most High) states: ‘And a tongue and two lips?’ [Quran, Surah Balad, 90:9] The taste papillae under the mucous membrane of the tongue have taste buds. There are different types of taste papillae: fungiform papillae, circumvallate papillae and foliate papillae. Fungiform papillae contain 200 – 400 sensory cells on the surface of the tongue on the tip and near the edge. They also have sensory cells for touch and temperature. Circumvallate papillae are at the base of the tongue and have V-shaped sensory cells. Foliate papillae are on the rear edges where there are around 20 with a few hundred taste buds in each (InformedHealth.org, 2016). The gustatory/sensory cells in the taste buds are connected to nerve fibres and form flower-shaped capsules that have a fluid-filled funnel containing finger-like projections called taste hairs (InformedHealth.org, 2016). The proteins on the surface of the hair fuse with chemicals for tasting. Amongst the taste buds are sour, sweet, salty, bitter and; umami (InformedHealth.org, 2016). The remainder of the taste buds function in the intensity of the taste, for instance, how sweet or sour something is. Many assume that spicy is also deemed as a taste but is classified as a pain signal. The sensation of sweetness is caused by the presence of fructose and lactose and other derivatives that activate sensory cells. Food that has acidic solutions, for instance, lemon juice and organic acids contain hydrogen ions dissolved in aqueous solution. The savoury taste can be described as meat broth by the presence of glutamic or aspartic acid. The mineral salts of potassium, sodium and magnesium enable the sensation of saltiness to occur. This is a similar case with bitter food that provide a bitter sensation (InformedHealth.org, 2016). The teeth help to grind the food and spread the aroma around the mouth. Cleaning the teeth is part of health and well-being. It has been advised that during the following five scenarios it is mustahabb (recommended): when the teeth are yellow, the breath of mouth changes, when waking up, praying and performing ablution (Ibn Abidin, 1979). The Prophet (peace be upon him) used a wooden stick called miswak to clean the mouth during the morning and night. Some were unsure of how many times he utilized it (Omar and Ibn Hanbal' 2004). He said in a hadith: Prophet Muhammad (peace be upon him) said: “Use miswak. Certainly, miswak is a cleansing for the mouth.” [Bukhari, Nasai', Ibn Majah] Today, many observe this as part of Sunnah and; we are advised to utilize fluoride-based toothpaste daily. Oral care is fundamental to prevent dental caries that is still amongst one of the major public health issues (Kanduti et al. 2016).  Figure 7: The anatomy of the oral cavity. (Kraan et al. 2014). The sensory pathway of taste The perception of taste is facilitated with the brain where the smell of the food is sent to the olfactory cortex. The texture and the feeling when touching also contribute to the taste (Kraan et al. 2014). The hydrophilic molecules in the food dissolved in the saliva stimulate the gustatory cells inside the taste buds in the oral activity. This stimulates the taste receptors where the peripheral information is sent to nerve fibres in the vagus, facial and glossopharyngeal nerves that associate with the brain stem (Vincis and Fontanini, 2019). They then transmit the signals to the medulla oblongata relaying them to the thalamic, subcortical and the cerebral cortex of the brain. The cerebral cortex (grey matter), subcortical (white matter) and the basal ganglia form the cerebral hemispheres. The convergence and divergence of information are then integrated into the central nervous system with the sensory system and the homeostatic, visceral and other processes ( Vincis and Fontanini, 2019). The power of touch Temperature, vibration, pressure, pain, the texture of an object are all different tactile sensations that can be felt via various receptors on the skin and relays the signal and travels to the brain via the peripheral nerves and can influence the reaction. The skin has three fundamental layers: an outer epidermis, middle dermis and inner hypodermis as presented in Figure 8. Merkel cells are receptors found in the basal layer of the epidermis of the hands, external genitalia and the lips. Meissner corpuscles are situated in the upper dermis of the feet soles and tips of fingers where there is no hair. The Pacinian corpuscles, Merkel and Meissner corpuscles can sense the touch, vibration and pressure stimulus, for instance, pain, itch and avoiding speech. Allah (The Most High) states: "And indeed, every time I invited them that You may forgive them, they put their fingers in their ears, covered themselves with their garments, persisted, and were arrogant with [great] arrogance." [Quran, Surah Nuh, 71:7] Other features of the skin consists of: Krause end bulbs that sense coldness whereas Ruffini cylinders sense the heat (Al-Ghazal, 2006). Another example is when feeling the pain stimulus, in the earlier generations, it was thought that the whole body senses the pain stimulus. However, the transmission of the pain and heat sensation from the nerve endings of the skin to the brain was later discovered. There are two types of afferent systems that elucidate pain sensations: epicritic and protopathic (Head, 1920; Price, 2007). Epicritic pain is localised and can sense a prick of a needle, or a slight alteration of temperature (Price, 2007). On the other hand, protopathic pain has a slow onset that can constantly feel pain repeatedly (Head, 1920). However, pain cannot be felt nor processed to the brain if the nerve endings are damaged, for example, after burning your hand severely. Allah (The Most High) states in the following verse: "Those who disbelieve in Our verses, We will drive them into a fire, every time their skins are roasted We will replace their skins with other new skins so that they may taste the torture. Allah is ever Exalted in Might and Wise." [Quran, Surah Nisa, 4:56] Al-Ghazal (2006) emphasised in relation to this verse that due to the severity of the nerve endings, those who enter the Fire cannot feel pain as it is not transmitted to the brain. This is why the burnt skin is replaced with fresh skin to feel the pain sensation. This further highlights the authenticity of the Quran that highlights this physiological and scientific fact before discoveries of man. Moreover, our fingerprints are unique even with monozygotic twins and have been mentioned by Allah (The Most High) centuries ago. Scholars have mentioned that they recreated people based on the fingertips that include the DNA. Allah (The Most High) states: " Yes indeed; We can reconstruct his fingertips. On Resurrection Day, Allah will reconstruct our bodies to the smallest detail even our unique fingerprints." .[Quran, Surah, Verse 4]  Figure 8: The structure of the skin (Lihacova, 2015) The power of proprioception Proprioception otherwise known as kinaesthesia is considered the sixth sense. It focuses on position, movement and balance of our limbs, muscles and joints and this in turn; allows people to touch (Proske and Gandevia, 2012). So why is it not considered a touch sense? Proprioception is the ability to sense muscle force, weight, effort, viscosity and movement as opposed to what it touches, for instance, texture, feeling and signals of pain. Allah (The Most High) states: “And [mention, O Muhammad], the Day when the enemies of Allah will be gathered to the Fire while they are [driven] assembled in rows. Until, when they reach it, their hearing and their eyes and their skins will testify against them of what they used to do. And they will say to their skins, "Why have you testified against us?" They will say, "We were made to speak by Allah, who has made everything speak; and He created you the first time, and to Him you are returned. And you were not covering yourselves, lest your hearing testify against you or your sight or your skins, but you assumed that Allah does not know much of what you do” [Quran, Surah Fussilat 41: 19 – 22] In our body, there are three types of muscle tissues: skeletal, cardiac and smooth muscles. The morphology of the muscle fibres differs in each type. The cardiac muscle is striated and arranged in bundles. It has an involuntary control mechanism and resides in the heart to help circulate blood around the body. There are mitochondria in the cells required for respiration. Similarly, skeletal muscles also have a striated feature and are essential for voluntary movement where it is attached to the muscle via the tendon. The skeletal muscle has repeated thin spherical long chains of the actin protein filaments and is surrounded by thick protein filaments (myosin) to create the bundling feature and; slide passed each other for the muscles to contract. The thin actin filaments have a myosin-binding site which allows the spontaneous bonding with myosin to occur. When the myosin binds, it undergoes a conformational change and; this causes the thin filament to move. The thin filaments are attached to a dense protein plate called a Z disc that anchors them. On the other hand, the smooth muscle has a striated feature and functions in protecting internal organs such as the stomach and provide involuntary muscle contractions. The sensory pathway of proprioception There are kinaesthetic receptors/mechanoreceptors to detect stretch and other movements in the effector muscles, skin, tendons and joints. The signal is transmitted to the motor input to control movement (Taylor, 2009). The afferent nerves affect the tone and postural reflexes (Aman et al. 2014). The proprioceptive sensations differ from the exteroceptors in the ear and eye (Proske and Gandavia, 2012). Thixotropy allows tension and stiffness that is exhibited by the muscle spindles and the skeletal muscles. Input from primary endings of muscle spindle aid in the position and movement; whereas secondary endings of the muscle spindles are linked to a sense of position (Tsay et al. 2015).  Figure 9. The sensory pathway of propriception (Cummings, 2004) Overall, we have six senses: hearing, sight, smelling, taste, touch and proprioception where they transmit the peripheral information to the brain to facilitate how we perceive the world around us. Advancement in neuroimaging, for instance, magnetic resonance imaging (MRI) assists in observing the proprioceptive stimuli and the integrative input of other senses. This has all been created by Allah (The Most High) and; we will be accountable for what we do with our senses. Our physical and spiritual senses interrelate our behaviour, emotions and thoughts. A combinatorial approach in the Quran, Sunnah, Medicine and Science teaches the knowledge, spiritual and moral doctrines to learn and understand the human senses how to use our six senses, manage it with responsibility and provide benefits to humanity (Fathil et al. 2015). Next month, I aim to go more in-depth with the anatomy and physiology of the brain and what evidence in the Quran and Sunnah that associates with it.  References Alberti, P. (2006) The Anatomy And Physiology Of The Ear And Hearing https://www.who.int/occupational_health/publications/noise2.pdf
Allen, F. and Schwartz, M., (1940) The Effect Of Stimulation Of The Senses Of Vision, Hearing, Taste, And Smell Upon The Sensibility Of The Organs Of Vision. The Journal of General Physiology, 24(1), pp.105-121. Al-Ghazal, S. (2006) Medical Miracles of the Quran. UK: Islamic Foundation. Al-Nahlawi, A.R. (1983). The principle of Islamic education and its methods. Syria: Dar al-Fikr Alper, C., Luntz, M., Takahashi, H., Ghadiali, S., Swarts, J., Teixeira, M., Csákányi, Z., Yehudai, N., Kania, R. and Poe, D., (2017) Panel 2: Anatomy (Eustachian Tube, Middle Ear, and Mastoid—Anatomy, Physiology, Pathophysiology, and Pathogenesis). Otolaryngology–Head and Neck Surgery, 156(4_suppl), pp.S22-S40. Altundag, A. and Cayonu, M., (2016) Chemical Senses in Cancer Patients. Current Pharmaceutical Design, 22(15), pp.2264-2269. Aman, J., Elangovan, N., Yeh, I. and Konczak, J., (2015) The effectiveness of proprioceptive training for improving motor function: a systematic review. Frontiers in Human Neuroscience, 8. p1075 Bishop, B. (1980) Pain: its physiology and rationale for management. Part I. Neuroanatomical substrate of pain. Physical Therapy 60 (1) pp.13-20. Blaus, B. (2020) Anatomy of the Eye Image Available [online] http://www.digitaljournal.com/topic/Anatomy%20of%20the%20Eye Catala, M. and Kubis, N. (2013) Gross anatomy and development of the peripheral nervous system. Handbook of Clinical Neurology 115 pp. 29-41. Cauna N. (1982) Blood and nerve supply of the nasal lining. In: Proctor DF, Anderson IB, ed. The nose. Amsterdam: Elsevier Biomedical Press; p. 45–70. Chaudhary, Y (2020) Tadabbur (Reflecting upon the Qur’an Series) Available [online] https://sacredtexts.co.uk/2018/05/28/tadabbur-reflecting-upon-the-quran-2/ Cohen, B. (2013) Paediatric Dermatology 4th ed. Available online: https://www.sciencedirect.com/topics/medicine-and-dentistry/oral-cavity Connel, D.C. and Fregosi, R.F. (1993) Influence of nasal airflow and resistance on nasal dilator muscle activities during exercise. Journal of Applied Physiology 74 pp. 2529–2536. Dar al-Iftaa Al-Missriyyah (2020) What bearings do visions have in Islam?Available [online] https://www.dar-alifta.org/Foreign/ViewFatwa.aspx?ID=5839 Dion, M.C, Jafek, B.W and Tobin, C.J. (1978) The anatomy of the nose: external support. Archives of Otolaryngology 104 pp. 145–150. Dubin, A. and Patapoutian, A. (2010) Nociceptors: the sensors of the pain pathway. Journal of Clinical Investigations 120 (11) pp. 3760-72 Farjo, A.A, McDermott, M.L. and Soong, H.K. (2009) Corneal anatomy, physiology, and wound healing. In: M Yanoff, JS Duker, eds. Ophthalmology, 3rd ed. Edinburgh, Mosby Elsevier: Elsevier Inc., pp. 203– 8. Fathil, Mohd & Saam, Zulfan & Sukendi, Sukendi & Nizar, Syamsul. (2015). Islam and the Environment: Education Perspective. AL-Ta lim. 22. 96. 10.15548/jt.v22i2.128. Fulkerson, M., (2014) Rethinking the senses and their interactions: the case for sensory pluralism. Frontiers in Psychology, 5. p.1426. Gadhvi M and Waseem M. (2020) Physiology, Sensory System. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; Available from: https://www.ncbi.nlm.nih.gov/books/NBK547656/ Garrity, J. (2020) ‘The Optic Pathway’ Available online: https://www.msdmanuals.com/en-kr/professional/eye-disorders/optic-nerve-disorders/the-optic-pathway Geurkink, N., (1983) Nasal anatomy, physiology, and function. Journal of Allergy and Clinical Immunology, 72(2), pp.123-128. Ghanty, I. and Schraag, S., (2019) The quantification and monitoring of intraoperative nociception levels in thoracic surgery: a review. Journal of Thoracic Disease, 11(9), pp.4059-4071. Head, H. (1920) Studies in Neurology. London: Oxford University Press. Ibn Abidin, M. (1979) Radd Al-Mukhtar ala Durr al-Mukhtar Sharh Tanwir al-Absar Beirut: Dar al-Fikr. Ibn Qayyim Al-Jawziyah, M. (1991) Al-Wabil Al-Sayyib wa Rafi Al Kalim Al-Tayyib Cairo: Dar Al-Hadith. Ibn Qayyim Al-Jawziyah, M. (2018) Madarij Al-Salikin: Bena Manazil Iyyak Na’bood wa iyyak Nastaeen (Ranks of The Divine Seekers). Dar Al Hadith Ibn Sina (1952) Avicenna's Psychology: An English Translation Of Kitab Al-Najat, Book 2, Chapter 6; With Historico-Philosophical Notes And Textual Improvements On The Cairo Editon London: Oxford University Press. InformedHealth.org (2016) How does our sense of taste work? Institute for Quality and Efficiency in Health Care (IQWiG). Irvine, K. and Clark, J., (2017) Chronic Pain After Traumatic Brain Injury: Pathophysiology and Pain Mechanisms. Pain Medicine, 19(7), pp.1315-1333. Jones, N., (2001) The nose and paranasal sinuses physiology and anatomy. Advanced Drug Delivery Reviews, 51(1-3), pp.5-19. Kanduti, D., Sterbenk, P. And Artnik, B (2016) Flouride: A Review of use and effects on health. Mater Sociomedicine. 28 (2) p. 133-137. Knight, J., Wigham, C. and Nigam, Y. (2017) Anatomy and physiology of ageing 6: the eyes and ears. Nursing Times [online]; 113: 7, 39-42. Kraan, H., Vrieling, H., Czerkinsky, C., Jiskoot, W., Kersten, G. and Amorij, J., (2014) Buccal and sublingual vaccine delivery. Journal of Controlled Release, 190, pp.580-592. Lihacova, Ilze. (2015). Evaluation Of Skin Oncologic Pathologies By Multispectral Imaging Methods. 10.13140/RG.2.2.12585.70242. Masland, R.H. (1986) The functional architecture of the retina. Scientific American; 255 pp.102– 11. McWilliams, M. (2008) Foods: experimental perspectives. 6th ed. Ohio: Pearson Prentice Hall p. 45-52. Muhamad, A., Syihab, A.H. and Ibrahim, A.H. (2020) Preserving Human–Nature’s Interaction for Sustainability: Quran and Sunnah Perspective. Science Engineering Ethics 26, pp. 1053–1066. Müller, L.J, Marfurt, C.F, Kruse, F., Tervo, T.M.T. (2003) Corneal nerves: structure, contents and function. Experimental Eye Research; 76 pp. 521– 42. Omar, A. And Ibn Hanbal, A. (2004) Imam Ahmad Bin Muhammad Bin Hanbal: USA: Noor Foundation. Price D. (2007) First and Second Pain Assessment (First Pain, Pricking Pain, Pin-Prick Pain, Second Pain, Burning Pain). In: Schmidt R., Willis W. (eds) Encyclopedia of Pain. Springer, Berlin, Heidelberg. Proctor, D.F. and Adams, GK III. (1976) Physiology and pharmacology of nasal function and mucus secretion. Pharmacological Therapy. 2 pp. 493–509. Proske, U. and Gandevia, S., (2012) The Proprioceptive Senses: Their Roles in Signaling Body Shape, Body Position and Movement, and Muscle Force. Physiological Reviews, 92(4), pp.1651-1697. Ranson, S.W. and Clark, S.L (1959) Anatomy of the Nervous System. Philadelphia: WB Saunders Co. Rehwaldt, M, Wickman, R, Purl, S, Tariman, J, Blendowski, C., Shott, S., Lappe, M. (2009). Self-care strategies to cope with taste changes after chemotherapy. Oncology Nursing Forum. 36(2): E47-E56. Richardson, J., Holmes, E. And Mueller, W., (1939) Anatomy And Physiology Of The Ear. Archives of Otolaryngology - Head and Neck Surgery, 29(3), pp.560-577. Sabale, A., Kulkarni, A. and Sabale. (2020). Nasal In Situ Gel: Novel Approach for Nasal Drug Delivery. Journal of Drug Delivery and Therapeutics. 10. 183-197. 10.22270/jddt.v10i2-s.4029. Sahin-Yilmaz, A. and Naclerio, R., (2011) Anatomy and Physiology of the Upper Airway. Proceedings of the American Thoracic Society, 8(1), pp.31-39. Sawaluddin, S., Hitami, M., Darussamin, Z. and Sainab, S., (2018) The Potential of the Senses in Al-Quran as the Basic Elements of the Human Physic and Its Application in Learning. Proceedings of the International Conference on Islamic Education (ICIE 2018). Schiffman, SS. (2007) Critical illness and changes in sensory perception. Proceedings of the Nutrition Society. 66: 331-345. Schubert, H.D. (2009) Structure and function of the neural retina. Marmor MF. Retinal pigment epithelium. Roh S, Weiter JJ. Retinal and choroidal circulation. In: M Yanoff, JS Duker, eds. Ophthalmology, 3rd ed. Edinburgh, Mosby Elsevier: Elsevier Inc., pp. 511– 21. Sempo, M., Salam, R., Mohd, R., Zainudin, W., Zainol, Z., Zaki, Z., Ibrahim, M. and Sayuti, M., (2017) The Quranic Philosophy on Superiority of Audio Sense Against Visual Sense Based on the Book of Exegesis and Science Reports. Advanced Science Letters, 23(5), pp.4765-4768. Shannan, B. (2010) Audiology - A Curriculum for Excellence Available [online] http://www.ssc.education.ed.ac.uk/courses/deaf/dnov10i.html Sokolowski, B., (2007) Sensory Systems. xPharm: The Comprehensive Pharmacology Reference, pp.1-5. Taylor, J., (2009) Proprioception. Encyclopedia of Neuroscience, pp.1143-1149. Thanc Foundation (2020) Nose & Sinus Cancer Anatomy Available [online] https://thancguide.org/cancer-types/nose-sinus/anatomy/ Tsay, A., Giummarra, M., Allen, T. and Proske, U., (2016) The sensory origins of human position sense. The Journal of Physiology, 594(4), pp.1037-1049. van Stralen, H. E., and Dijkerman, H. C. (2011). Central touch disorders. Scholarpedia 6(10), 8243. Vincis, R. and Fontanini, A., (2019) Central taste anatomy and physiology. Handbook of Clinical Neurology, pp.187-204. Willoughby, C., Ponzin, D., Ferrari, S., Lobo, A., Landau, K. and Omidi, Y., (2010) Anatomy and physiology of the human eye: effects of mucopolysaccharidoses disease on structure and function - a review. Clinical & Experimental Ophthalmology, 38, pp.2-11. Zhu, J., Zhang, E. and Rio‐Tsonis, K., (2012) Eye Anatomy. eLS,.  The origin of human nature and how it developed is known as embryology. With today’s advanced imaging and analytical techniques and well-established genetic and experimental models, the development of invertebrates and vertebrates can be studied. The function of this section of my qualitative research review is to prescribe an understanding of how a human is traditionally reproduced and developed from a medical, scientific and Islamic perspective. The Quran and Hadith contain a multitude of evidence on developmental biology; which is a guide for the creation by the Creator, Allah (The Most High) who created man in the best possible manner. “Verily, We created man in the best statue (mould)” [Quran, Surah Tin, 95:4] However, the accuracy and thorough understanding of the Quranic verses and Hadith on the embryonic development were raised after significant discoveries from the ancient times to date have been made by many philosophers and scientists in explaining the key stages in how gametes formed to the full-term pregnancy (World Muslim League, 2000). This ultimately challenges any academic or expert in the field of embryology with such transparency and vivid description of the intrauterine life at the time of the Quran’s revelation; the seventh century where no technology existed. The creation and structure of the human body imply the infinite love of Allah (The Most High) for His creation (Hossain, 2018). Amongst the first philosophers who had an interest in embryology is Aristotle who utilized animal models, for instance, fish, snakes, turtles and insects to perform anatomical studies to discover the development of a human (Saadat, 2009). He compiled it in his book: ‘On the Generation of Animals’ ‘De generatione animalium’ (Boylan, 1984). He also revealed that the foetus is composed of menstrual blood formed in the uterus and is minuscule in the ovum or sperm. However, Allah stated in the following verse: “Was he not a drop of germinal fluid emitted?” [Quran, Surah Al-Qiyamah, 75:37] One of the prominent scholars, Ibn Hajar Al Asqalani (1997) stated that: “Many Anatomists claim that the male fluid has no effect on the creation of the child except for coagulation of blood and that the child is formed from the menstrual blood. However, the Prophet’s Hadith in this chapter refutes this claim”. The findings and conceptions of Aristotle were challenged by Galen because some eggs of models used fertilized, whereas other animals grew spontaneously from meat, for instance, flies (Saadat, 2009). In the second century, Galen described the structure and function of the placenta and the role of placental proteins in embryonic development in his book ‘On the formation of the foetus’ (Longo and Reynolds, 2010). Furthermore, the invention of the microscope by Zacharias Janssen in the sixteenth century which was further developed by Anton van Leewenhoek and Robert Hooke in the seventeenth century who invented the light and the compound microscopes respectively brought wonders of the natural sciences (Wollman et al. 2015; Hooke, 1665). The instruments led to ongoing discoveries and illustrations that contribute to the development of medical and scientific knowledge, particularly in embryology. In 1672, Malphigi studied poultry eggs under the microscope who questioned epigenesist and discovered muscle-forming somites (Keele et al. 1978; Gilbert, 2000). In 1775, Spallanzani revealed that the spermatozoon and ovum are required to fertilize for a human to be developed (Capanna, 1999). This highlight the progression of understanding embryology. Later in the 19th century, Frankie Lillie (1914) discovered the physical and chemical mechanisms in how the fertilization step takes place between the egg and the sperm. Today, researchers utilize various genetic techniques and advanced imaging tools to study the cells. However, the comprehensive methodology of how the human body developed is already present in the Glorious Quran. The Seal of the Prophets, Muhammad (peace be upon him) was illiterate and; he was taught by Allah (The Most High). It was through Prophet Muhammad (peace be upon him), many scholars sought advice on the Tafsir of the Quranic verses to develop their knowledge and understanding of Allah (The Most High) divine wisdom (Moore, 1986). Thus, with certainty, Allah has created human and monitored the reproduction and embryonic development phases until the baby enters Earth. The child then grows and lives and dies as he or she destined to be. Modern technology and knowledge cannot measure and understand the infinite dimensions in which this universe possesses. Allah (The Most High) manages all affairs who created everything with His Mercy, wisdom and intellect. The development of man consists of physical creation, spirit, fitrah and light (Shakir, 2018). The first person that landed on Earth was Adam (peace be upon him) and was physically created by Allah (The Most High) in His image with ‘Both His Hands’ as mentioned in the Tafsir of Ibn Abbas (may Allah have mercy upon him) in the following Quranic verse: “(He said) Allah said to him: (O Iblis!) O wicked one! (What hindereth thee from falling prostrate before that which I have created with both My hands) what prevented you from prostrating before that which I have shaped with My hands? (Art thou too proud) to prostrate before Adam (or art thou of the high) or are you of those who disobey My command?” [Quran, Surah Saad, 38:75] This emphasizes the great care in creating Adam without the intermediary of a mother nor father (Shakir, 2018). Some jurisprudence such as Abu Thawr and Ibn Khuzaymah explained that it was in Adam’s image (Melchert, 2011). The Ruh (spirit) comprises the senses, wisdom and physical stature of the humankind as mentioned in the following Quranic verse: “And when He had made him upright and breathed into him of His spirit” [Quran, Surah Saad, 38:72] In another narration, Allah (The Most High) states: "Thereafter, He moulded him and breathed into him of His Spirit, and He made for you hearing and beholding (s) (i.e., eyesight) and heart-sights; (i.e., perception) little do you thank (Him)." [Quran, Surah Sajdah, 32:9] This indicates that the spirit was breathed into the human body and soul. There are two types of spirits: Al-Sugrah where death occurs during the sleep and Al-Kubrah; the actual death. In each form, the spirit leaves the body but in Al-Sugrah returns (Setiawan et al. 2019). Al-Razi implied that once the spirit has entered the body, it travels to every part and described metaphorically as the air breathed into a vessel. The Fitrah (natural disposition) occurs from Allah (The Most High) and has several perspectives based on its etymology otherwise known as ‘lafaz al mushtarik’ (Rahman, 2012; Kamus Dewan, 1996). Al-Jurjani, (2003) stated that the Fitrah is the divine form created within the child in the womb of the mother where he or she accepts Islam as the religion of the truth by nature. Another understanding of its meaning is the inner consciousness of a person (Bhat, 2016). Ibn Manzur (1988) explained that when Allah blesses someone and grant them peace and teaches man to repeat certain words when lying down to sleep, that if one were to die the same night, one would die upon the truth; the fitrah. “So direct your face toward the religion, inclining to truth. [Adhere to] the fitrah of Allah upon which He has created [all] people. No change should there be in the creation of Allah. That is the correct religion, but most of the people do not know” [Quran, Surah Al Rum, 30:30] Amongst the 99 attributes of Allah (The Most High) is Al-Fatir, the creator and inventor who created the fitrah in man. Light also forms part of the human creation given from Allah (The Most High) as mentioned in the following verse below (Al-Razi, 2010): “On the Day you see the believing men and believing women, their light proceeding before them and on their right, [it will be said], "Your good tidings today are [of] gardens beneath which rivers flow, wherein you will abide eternally." That is what is the great attainment.” [Quran, Surah Hadid, 57:12] Therefore, the people who have affirmed their faith will be recognised by Allah (The Most High) and is based on their righteous deeds, the piety of their characters and this correlates with the luminous and intensity of the light. Ibn Kathir narrated that Abdullah ibn Masood (may Allah have mercy upon him) and collected by Ibn Abu Hatim and Al-Tabari that there will be light running forward before them. "They will pass over the Sirat according to their deeds. Some of them will have a light as large as a mountain, some as a date tree, some as big as a man in the standing position. The least among them has light as big as his index finger, it is lit at times and extinguished at other times.'' Therefore, the development of man consists of the physical creation and other dimensions highlighted. However, the scope of this section is to focus on the physical creation that associates medicine and science with the Glorious Quran. The formation of the human from clay The creation of man has been detailed throughout the Quran more than other creation as presented in Table 1. At first, the dust is mixed with water to form clay that was sticky and viscous. Based upon the chemical composition of clay we would discover various elements in the human body that assemble them such as carbonates, water-soluble salts, minerals such as silicon, calcium and iron (Vakalova et al. 2018). It was informed by Ibn Manzur (2010) that the term Lazeeb is extracted from the term lazooba which means a sticky solid. The sticky product is then converted into muntin stinking. Muntin is thin strips of wood that divide the glass panels. Allah (The Most High) uses the term Al hama which is a form of black mud and has turned to masnoon due to a change in water. When mixing it with sand, it forms a ‘salsal' which is dried clay and this has been agreed by various scholars (Ibn Manzur, 1988; Al-Razi, 2010).  Figure 1: The process of the formation of sounding clay Therefore, our Prophet Adam (peace be upon him) was formed from sounding clay that is black, soft mud that has altered. Ibn Jarir, Ibn Qayyim Al Jawziyah and Qatadah Ibn Dia’amah Sadusi Basri and other scholars agree with this. Ibn al-Qayyim Al Jawziyah (1960) said: “When the perfection, complete power, all-encompassing knowledge, ever-executed will and utmost wisdom of the Lord decreed that His creation should be of materials of different kinds and that they should vary in their forms and attributes and natures, His wisdom decreed that He should take a handful of dust from the earth, then mix it with water. So it became like black stinking mud. Then the wind was sent upon it and it dried out until it became clay-like pottery. Then it was given shape and limbs and faculties, and each part of it was given a shape suited to its purpose”. Abu Musa Al-Ashari (may Allah have mercy upon him) who said: “I heard the Messenger of Allah (peace and blessings of Allah be upon him) say: ‘Allah created Adam from a handful that He gathered from the entire earth, so the sons of Adam come to like the earth. Some of them are red, some are white, some are black and some are in between. Some of them are easy, some of them are difficult, some are evil and some are good.” [Al-Tirmidhi, 2955; Abu Dawood, 4693] This evidence provides an insight into the morphogenesis of the materials and architecture in how Allah (The Most High) has created Adam (peace be upon him) in the shape and form He desires. The first human created and generations upon generations initiated. However, human development does not pause at the clay. For Allah (The Most High) states in the Quran: "And indeed We created man (Adam) out of an extract of clay (water and earth); Thereafter We made him (the offspring of Adam) as a Nutfah (mixed drops of the male and female sexual discharge and lodged it) in a safe lodging (womb of the woman); Then We made the Nutfah into a clot (a piece of thick coagulated blood), then We made the clot into a little lump of flesh, then We made out of that little lump of flesh bones, then We clothed the bones with flesh, and then We brought it forth as another creation. So Blessed is Allâh, the Best of creators" [Quran, Surah Al Muminoon 12-14] The transitional changes and time intervals from one developmental phrase from one stage to another are emphasised with total accuracy by Allah (The Most High) by the phrase ‘then' where the clay extract to a drop from the spermatozoon ‘mixes' or fertilises the egg from the ovum to become a zygote (An-Najjar, 2005). At the end of the clot phase, researchers have staged that somites are formed and converts into a Morsel giving the embryo shape. The ‘lump' of flesh form the appendicular and axial skeletons via osteogenesis. The axial skeleton consists of ribs and the cartilaginous vertebral column derived from the sclerotome (Dockter, 1999). The formation of sclerotome and somite chondrogenesis stimulated by two ligand molecules, Noggin and Shh in the notochord and neural tube (Dockter, 1999). The bones are ‘clothed' with flesh (muscle and skin); the dermomyotome. Dermomytome is an epithelial cell layer situated at the dorsal end of the somite which aid in the formation of the dermis and skeletal muscle of the myotome ontogeny and tissues (Ganten et al. 2006). By understanding the morphogenesis, one can understand the underlying processes involved in carcinogenesis, wound healing and organ regeneration (Sieck, 2019; Kahane et al. 2013). Table 1: Some of the Quranic evidence of human created from clay.  An insight into the Nutfah (zygote phase) Following the formation of the clay, Nutfah occurs where one male germ cell, spermatozoa required to ejaculate during sexual intercourse to penetrate and fuse with the ovum, the female sex cell to produce a fertilized egg called the zygote. To conceive twins depends on the genetic disposition and environmental factors (Hoekstra et al. 2008). Monozygotic twins are genetically identical and are caused from one zygote and divided into two where they commonly have two amnions, one chorion and one placenta (Hoekstra et al. 2008). On the other hand, dizygotic twins have two zygotes independently fertilized where the outcome consists of two of each of the following: amnions, chorions and placenta where there is ca. 65% of is fused (Hoekstra et al. 2008). Allah (The Most High) described the formation of the zygote in the following verses that a small quantity of both secretions required during the Nutfah phase called Amshaj. The fluid is discharged from both men and women to fertilize in the fallopian tube before descending to the uterus where implantation occurs followed by the development of villosities called Alaq (Sadaat, 2009). William Harvey’s doctrine omne vivum ex ovo translates to all life comes from the egg highlights the importance of the egg and sperm evading the theory of spontaneous generation (Keynes, 1966). Understanding the embryological phases from fertilization to birth through the Quranic verses supplemented with the modern medical and scientific evidence provides us with an anatomical and physiological understanding us to know how we all started (Varga, 2017). “And that He creates the two mates - the male and female. From a sperm-drop when it is emitted” [Quran, Surah Al-Najm, 53:45–46] “Verily, I created humankind from a small quantity of mingled fluids.” [Quran, Surah Insan, 76:2] “And it is He Who has created man from water, and has appointed for him kindred by blood, and kindred by marriage” [Quran, Surah Al Furqan, 25:54] “Then He made his offspring from semen of despised water (male and female sexual discharge)” [Quran, Surah Al-Sajdah, 32:8]. The Amshaj consists of three phases: Khalk, Taqdir and Harth (Sadaat, 2009). Khalk is the fertilization process where the zygote has 46 chromosomes. There are two types of cell division: meiosis and mitosis. Meiosis is derived from the Greek word mitos meaning thread which describes the thread-like appearance of the chromosomes (Albert et al., 2002). It is a regulated process that consists of two successive rounds of cell division to create gametes. Meiosis differs from mitosis in the regulatory mechanisms but is similar in the process of segregation and recombination (O’Connor, 2008). Allah (The Most High) has designed the female and male reproductive systems whose function is to produce these gametes and hormones and support the development of the foetus and delivering it to this enigmatic world (Betts et al., 2013). The female reproductive system situated in the pelvic cavity where the gamete produced is called an oocyte. Oogenesis initiates in the oogonia, where the primordial follicles develop in the primitive ovarian stem cells and; the primary oocytes form via mitosis before birth. They are then arrested during the first meiotic division and then reinitiates during puberty and continues until the menopause stage (Betts et al. 2013). The release of the oocyte signifies the conversion from puberty to a woman known as ovulation. It is estimated that the number of primary oocytes decreases from ca. two million to 400,000 at puberty and then zero post-menopause (Betts et al. 2013; Edwards et al., 1969). “And Allah has made for you from yourselves mates and has made for you from your mates sons and grandchildren and has provided for you from the good things. Then in falsehood do they believe and in the favour of Allah they disbelieve?” [Quran, Surah Al Nahl, 16:72] 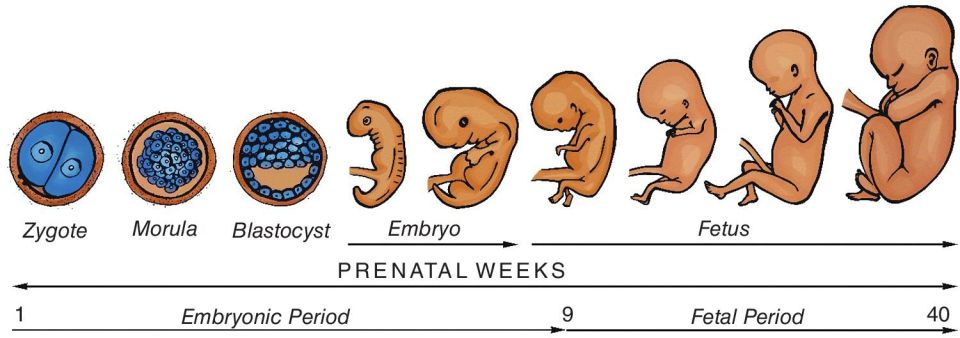 Figure 2: A schematic presentation of the meiotic process (Marston and Amon, 2005) The second phase of the Amshaj is the formation of facial and other characteristics and is called Taqdir (Sadaat, 2009). The determination of the gender can be identified depending on the type of chromosome that fertilizes the ovum and is facilitated by the cascade of factors induced by the SRY (Sex-determining region of the Y chromosome) (Betts et al. 2013). The male gender has an XY chromosome whereas, a female has an XX chromosome. If the Y chromosome of the man fertilizes the ovum it is a boy and if it is an X chromosome it is a girl. In the female and male embryos, the tissue is bipotential where the cells can differentiate to form female or male gonads (Betts et al. 2013). This causes a series of cascade where functional SRY gene causes the individual to become a male and, when it is not functional it becomes a female to form spermatogonia and oogonia respectively. The bipotential paradigm can be explained with testosterone where Leydig cells secrete the hormone that can directly differentiate into glans penis present in the male reproductive system or the glans clitoris in the female reproductive system. However, without testosterone, cells differentiate into the clitoris (Betts et al., 2013). Moreover, sustentacular cells also secrete testosterone which stimulates the growth of the male duct, Wolffian and degrades the female duct; Mullerian duct; low levels of testosterone causes the production of the Mullerian duct (Betts et al. 2013). This signifies the significant impact that hormones have to mature reproductive system and develop sexual characteristics. Besides testosterone and oestrogen from the gonads, the luteinizing hormone (LH) functions synergistically with follicle-stimulating hormone (FSH) to induce the growth of follicles and ovulation; they are both secreted in the anterior gland (Raju et al. 2013). The Gonadotropin-releasing hormone (GnRH) is secreted from the hypothalamus and determines the secretion of both LH and FSH that function in maturing the gonads (Marques et al. 2018). “God fashioned humans from a clinging entity.” [Quran, Surah Alaq, 96:2] On the other hand, the bipotential mechanism of differentiation of internal structures of the reproductive system is not apparent in all tissues. For instance, the uterus found in the female and the ductus deferens, epididymis and seminal vesicles in males are derived and produced from one of the duct systems of the embryo (Betts et al., 2013). For it to be functionally active, one must develop appropriately whilst the other degrades (Betts et al., 2013). From an Islamic perspective, Allah (The Most High) has informed us that Eve has been created from the rib of Prophet Adam (peace be upon him) and is has caused significant discussions amongst the scholars of the exegesis. However, it is important to state that within the legal theory, Usul Al-Fiqh, there are several laws of language, Quwaid Al-Lughawiyah, for instance, clarity (Al-Faz Wadihah), reference (Turooq Al-Fiqh), pronunciation (lafz) and qualities (sighaat) to understand the basics and phrases present in Quran and Hadith (Al-Shami, 2015; Zulkifli, 2017). In Surah Al Zumr, Allah says ‘He created you from one soul’ and exemplary scholars such as Al-Tabari (2000), Al-Razi (1981), Ibn Asyur (1984), Al-Suyuti and al-Mahalli, (2007), Ibn Kathir (1980) and Ibn Kathir (2014) explains that the one soul is Adam and the mate is Eve. Therefore, Eve was produced from the left rib of Adam whilst he was asleep. However, Ibn Kathir (1980) does not elaborate on how Eve was created as that of Adam from clay to birth which indicates that they undergo the same process of pregnancy. “It is He who created you from one soul and created from it its mate that he might dwell in security with her. And when he covers her, she carries a light burden and continues therein. And when it becomes heavy, they both invoke Allah, their Lord, "If You should give us a good [child], we will surely be among the grateful." [Quran, Surah Al Araf, 7:189] “O mankind, fear your Lord, who created you from one soul and created from it its mate and dispersed from both of them many men and women. And fear Allah, through whom you ask one another, and the wombs. Indeed Allah is ever, over you, an Observer.” [Quran, Surah Al Nisa, 4:1] “He created you from one soul. Then He made from it its mate, and He produced for you from the grazing livestock eight mates. He creates you in the wombs of your mothers, creation after creation, within three darknesses. That is Allah, your Lord; to Him belongs dominion. There is no deity except Him, so how are you averted?” [Quran, Surah Al-Zumr, 39:6] On the other hand, some scholars disagree that Eve was created in this manner. For instance, Al Maraghi (1946) wherein the following verse in Surah Taha: “Thereof (the earth) We created you, and into it We shall return you, and from it, We shall bring you out once again” [Quran, Surah Taha, 20:55] The term we highlight that Adam and Eve created from the same material, earth. Another scholar, Al-Qismi, opposes the idea of Eve produced from Adam’s rib but of human nature (Al-Qismi, 2003). On the contrary, scholars such as Al-Kirmani (1981) emphasises that Eve created from the rib based on the following hadith that graded as sahih in Ale-Shaikh (2010) publication called Al-Kutub Al Sittah that comprises a compilation of six volumes of hadith: Al-Bukhari, Al Nisai, Muslim, Abu Dawood, Tirmidhi and Ibn Majah. Abu Hurairah (may Allah be pleased with him) narrated that Prophet Muhammad (peace be upon him) wherein the upper area of the rib there is crookedness that can is broken if straightened said: “Treat women kindly, for the woman was created from a bent rib, and the most crooked part of the rib is the top part, so treat women kindly.” [Al Bukhari and Muslim] A day after fertilization, the zygote divides (cleavage) into two cells without a cytosol, additional cleavage take place and, this causes a decrease in cell size per cell division. The cells that are dividing are known as blastomeres (Boiaini et al., 2019). The pre-implantation of the human embryo has two phases: the first three days occur in the fallopian tube and four days in the uterus. In total, the pre-implantation period is a week and; the outcome is a blastocyst implanted into the fundus of the uterine wall (Leese, 2010). This is known as Harth (Saadat, 2009). The zygote descends from the fallopian tube (oviduct) by peristalsis and cilia to the uterus where it is implanted in the endometrium by digesting the endometrial cells to a position in the uterine mucosa (Saadat, 2009). Implantation stimulated by the trophectoderm (TE) cells of the blastocyst (Hyun et al. 2020). The hormones, progesterone, oestrogen and human chorionic gonadotropin (hCG) are produced by the differentiated syncytiotrophoblasts to maintain the development of the embryo (Nwabuobi et al. 2017). On the fourth day, a 16 -32 cell conceptus formed towards the uterus where it appears like a solid mass comprising of blastomere within the zona pellucida; a glycoprotein layer around the embryo. This is called the morula as illustrated in Figure 3 and, there are two rounds of asymmetric divisions (Saini and Yamanaka, 2018). At the fourth cell division, the cell number increases from 8 to 16 and in the fifth cell division, 16 – 32 cells (Saini and Yamanaka, 2018). The conceptus that consists of the embryo and the additional membranes increase in cell number and nourished by the uterine milk secretions from the decidual cells of the endometrium; it is also mediated by progesterone (Ing et al., 1989). The endometrial secretion also causes the uterine lining to thicken (Ing et al., 1989). 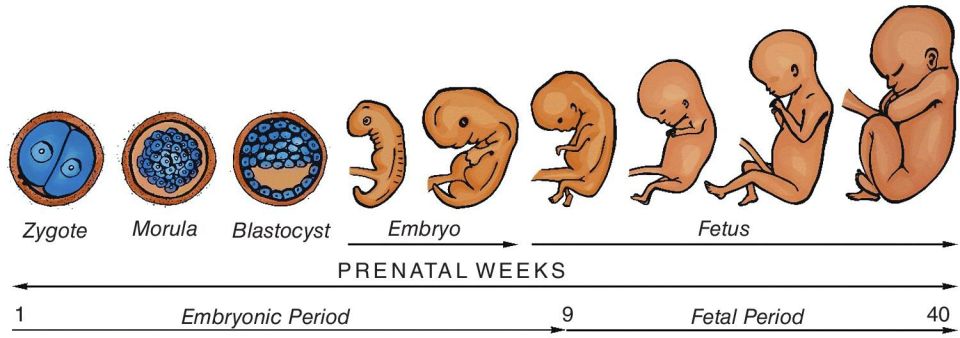 Figure 3: The embryological phases during the embryonic period and foetal period (Pocket Dentistry, 2017) An insight into the Takhliq phase (embryonic phase) Takhliq is organogenesis where differentiation from cells produces rudimentary structures of tissues and organs (Saadat, 2009). This takes place between the third and eighth week of gestation from germ layers: endoderm, ectoderm and mesoderm (Saadat, 2009). This stage extends from the beginning of the third week to the eighth week of the embryonic period: Alaqah (leech-like), Mudghah (somites), Idham (bones) and Laham (muscles) (Saadat, 2009). Alaqa phase There is several meaning of alaqa: leech, blood clot and a suspended substance and be explained as we go through the embryonic phase (Sadaat, 2009; Moore, 1986). On the fifth day, a transition takes place from a morula to blastocyst and is supplemented by a change in the metabolic pathway from pyruvate and lactate to glucose (Kaneko and DePamphilis, 2013). The formation of the blastocyte otherwise, known as blastula is necessary to determine the mammalian ontogeny and surrounded by a fluid-filled cavity called a blastocoel (Denkey, 1969; Kaneko and DePamphilis, 2013). The blastocyst consists of an inner cell mass (ICM) and trophectoderm (TE) (Marikawa and Alarcon, 2009). As the ICM increase in size, the zona pellicuda becomes thinner and hatches away from the zona pellicuda in the following day (Shafei et al., 2017). The ICM has totipotency of differentiating to various types of cells. For instance, the epithelial cells of the placenta, trophoblasts that surround the outer shell is maintained by the Hippo signalling pathway (Saini and Yamanaka, 2018). Both types of trophoblasts, cytotrophoblasts and syncytiotrophoblasts differentiate to form the chorionic membrane that positions the conceptus into the endometrium and form the foetal part of the placenta (Denker, 1969). The maternal part of the placenta-derived from the deepest layer of the endometrium; decidua basalis and the cytotrophoblasts remodel the maternal blood vessels that surround the chorionic villi and form the chorionic sac which extends into the endometrium (Gest, 2000; James, 2014). The mesenchymal cells from the mesoderm villi differentiate into umbilical blood vessels to connect the embryo with the placenta and allow the exchange of nutrients and removal of waste (Niakan et al. 2012). This is why this phase is described as the blood clot and suspended substance whereby blood vessels a formed and the embryo associates with the placenta (Moore, 1986). On the sixth day, the blastula attaches to the endometrium of the uterine wall for two to three weeks until the 25th day where it appears a ‘leech-like structure’ (Sadaat, 2009; Moore, 1986). The embryo is compared to a leech parasite because the embryo derives blood from the decidua. This is similar to the leech with the host (Kuo and Lai, 2018). The invention of the microscope has facilitated medical scientists to examine the morphological structure of the embryo that could not be achieved in the 7th century due to the miniature size of the embryo during the earlier days of pregnancy (Moore, 1986). This correlates with the following verse, where Allah (The Most High) describes the embryo as a leech-like structure: ‘Then We made the sperm-drop into a clinging clot, and We made the clot into a lump [of flesh], and We made [from] the lump, bones, and We covered the bones with flesh; then We developed him into another creation. So blessed is Allah, the best of creators.’ [Quran, Surah Muminoon, 23:14] During the second week, the blastocyst differentiates into layers producing extraembryonic membranes, chorion, amnion, allantois and yolk sac to protect and support the embryo and ensure implantation takes place (Hyun et al., 2020). The ICM produces a two-layered embryonic disc, the upper layer, epiblast, surrounds the amniotic cavity to form an amnion comprising of fluid and maternal plasma. The hypoblast endoderm is present on the ventral end of the disc and forms the yolk sac with the extraembryonic mesoderm (Hafez, 2017). The chorion is a membrane that surrounds the other membranes whereas the allantois is an excretory duct of the embryo that forms as part of the bladder to remove metabolic waste (Muench et al., 2017). The yolk sac and allantois produces the umbilical cord and allows nutrients to reach the embryo via primitive blood circulation (Pansky, 1982). The germ layers formed are endoderm, ectoderm and mesoderm to shape the foetus (Rehman and Muzio, 2020). The bi-laminar germ disk becomes a tri-laminar germ disk in the third week via gastrulation where multipotency rather than totipotency to form an oval shape and primitive streak on the epiblast to proliferate and develop the structures in the embryo (embryology.ch, 2020a). The epiblast produces the ectoderm, the middle layer mesoderm and the endoderm replaces the hypoblast produces the yolk (Pilato, 2003). The endoderm further differentiates to form two tubes: the gastrointestinal and respiratory tube (Gilbert, 2000). The gastrointestinal tube buds several organs: liver, pancreas and the gall bladder, whereas the respiratory tube bifurcates into two tubes (Gilbert, 2000). Both tubes share an anterior structure known as the pharynx where further epithelial structures, for instance, thymus, thyroids, parathyroid glands and tonsils appear (Gilbert, 2000). The process of the development of organs and the central nervous system is called neurulation. 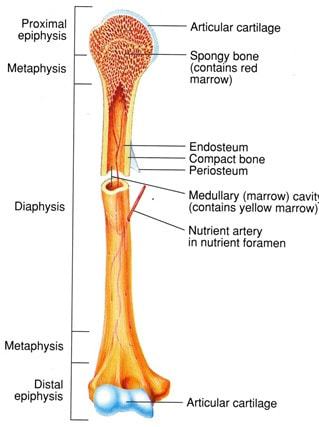 Figure 4: The embryo at 4 weeks during the first trimester (Shiel, 2009) Mudghah (Somites) phase. Following the alaqa phase, the development of the somites occurs and the embryo is described as a chewed up morsel (Moore, 1986). This is because of the small size (1 cm) and it can be chewable by teeth (Moore, 1986). It has a corrugated surface where some parts of the somites are formed and other areas are unformed that correspond to the differentiated and undifferentiated tissues (Sadaat, 2009). The primordial synthesis of the internal ears leads to the early creation of the eyes and then the brain (Moore, 1986). Allah (The Most High) has already started in the following Quranic verse of the transition between the alaqa to mughdah: “I fashioned the clinging entity into a chewed lump of flesh and I fashioned the chewed flesh into bones and I clothed the bones with intact flesh.” [Quran, Surah Al Muminoon 23:14] “O People, if you should be in doubt about the Resurrection, then [consider that] indeed, We created you from dust, then from a sperm-drop, then from a clinging clot, and then from a lump of flesh, formed and unformed - that We may show you. And We settle in the wombs whom We will for a specified term, then We bring you out as a child, and then [We develop you] that you may reach your [time of] maturity. And among you is he who is taken in [early] death, and among you is he who is returned to the most decrepit [old] age so that he knows, after [once having] knowledge, nothing. And you see the earth barren, but when We send down upon it rain, it quivers and swells and grows [something] of every beautiful kind.” [Quran, Surah Al-Hajj 22:5] In a hadith, Anas ibn Malik (may Allah have mercy upon him) narrated by the Prophet Muhammad (peace be upon him) said: “Allah has appointed an angel as the caretaker of the womb, and he would say: My Lord, it is now a nutfa or a sperm-drop; my Lord, it is now a clot; my Lord, it has now become a chewed morsel, and when Allah decides to give it a final shape, the angel says: My Lord, would it be male or female or would he be an evil or a good person? What about his livelihood and his age? And it is all written as he is in the womb of his mother.” [Al-Bukhari and Muslim] During the fourth week, the placenta decreases the size of the yolk sac to facilitate the blood vessels and the gametes. The connection between the placenta and the embryo via the umbilical cord is strengthened throughout the gestation period. The umbilical cord is a blood conduit with a helical and tubular structure that surrounds the amnion and is filled with the mesenchyme Wharton’s jelly; a supportive connective tissue (Spurway et al., 2012). It has one umbilical vein and two umbilical arteries but is not fully developed until the 12th week of the gestation (Jarzembowski, 2014; Spurway et al., 2012). The arteries remove deoxygenated blood into chorionic blood vessels and out of the chorionic villi where it filters the blood and exchanges nutrients and oxygenated blood between the foetal and maternal blood (Carlson, 2014; Denker, 1969). There are various mechanisms in how nutrients and drugs are exchanged, for instance, facilitated diffusion, active transport, passive transport and pinocytosis and the placental transfer rate is dependent on the molecular size and the pharmacological properties of the prescribed drugs (Griffiths et al., 2014). The placenta is permeable to lipophilic substances, for instance, antibiotics that move via facilitated diffusion, whereas it is hydrophilic to glucose and other small hydrophilic solutes (Faber and Anderson, 2012; Reynolds, 1998). Iron and amino acids are transferred by active transport (Faber and Anderson, 2012). Anaesthetic drugs and analgesic drugs can cross the placenta (Griffiths et al., 2014; Reynolds, 1998). The neuroectodermal cells that surround the embryo thicken and become a neural plate where tissues either side produces a neural tube (Pleasure et al. 2014). The neural tube transforms into a rod-shaped notochord and is then altered to a nucleus polposis of discs to facilitate in the generation of neurons (nerve cells) and neuroglial (supportive cells) via neuroepithelial progenitors (Pleasure et al. 2014). The two types of the nervous system, central nervous system (CNS) Aand the peripheral nervous system (PNS) are formed in the embryo at 18 days (Sadaat, 2009). Adhesion molecules, for instance, N-cadherin and neural cell adhesion molecule (NCAM) are transcribed to facilitate the development of the neural tube structure. Folate (Vitamin B12) is also essential for the neural tube where defects such as spina bifida and in severe cases anencephaly can occur in response to its deficiency (Molley et al. 2009). During the fifth week, the size of the neural tube increases at the anterior end and produces three primary vesicles of the brain: prosencephalon (forebrain), mesencephalon (midbrain) and rhombencephalon (hindbrain). The optic vesicles are also formed and extend laterally from the prosencephalon (Gilbert, 2000). This highlights how the ectodermal layer is fundamental for the development of the nervous system and the sensory epithelium of the various senses. Similar to brain development, the heart initiates as a primitive tube near the chorionic villi for contraction and conduction (Betts et al., 2013). The heartbeats during the fourth week but does not circulate the blood until the fifth week. The liver temporarily produces red blood cells until the bone marrow is fully developed. The heart is derived from the anterior splanchnic mesoderm and develops at the cardiogenic area of the embryo’s head (Groot et al. 2005). The cardiogenic area transitions to form two cardiogenic cords or cardiogenic plate following chemical signals from the endoderm that fuses in the midline to form a primitive heart tube (Betts et al., 2013; Groot et al. 2005). The primitive heart tube divided into transitional zones and primitive cardiac chambers. The chambers are primitive atrium, bulbus cordis, truncus arteriosis and primitive ventricle (Betts et al. 2013; Groot et al. 2005). The transitional zones are sinoatrial ring, sinus venosus, atrioventricular canal, primary ring and ventriculoarterial ring (Groot et al. 2005). During blood circulation, the venous blood travels into the sinus venosus from tail to head or from the sinus venosus to truncus arteriosis (Betts et al. 2013). Further developments occur until a full heart is formed whereby the truncus arteriosus is derived from neural crest cells transitions into the aorta blood vessel and pulmonary trunk, the bulbus cordis transitions into the right ventricle, the primitive ventricle forms the left side ventricle, the primitive atrium forms the left and right atria and two auricles. The sinus venosus forms the right atrium and sinus (Betts et al. 2013). On Day 23 – 28, elongation of the heart tube takes place which folds the pericardium which positions the chamber and vessels. The transitional zones assist in the development of the interatrial, interventricular and atrioventricular septa which positions and remodels the chambers, valves, differentiation of the conduction system and the fibrous heart skeleton (Betts et al. 2013; Groots et al. 2013). The process is facilitated by extracardiac cells: neural crest and epicardium derived cells (Groot et al., 2013). The heart formed by the end of 5th week, the atrioventricular and semilunar valves are produced between weeks 5-8 and 5-9 respectively (Betts et al. 2013). Significant embryonic folding longitudinal and transverse laterally takes place during the fifth week where the head and tail ends become apparent in a C-like shape (Sadaat, 2009). The body wall (somatopleure) folds within midline (Pansky, 1982). The gastrointestinal tract is amongst those that had significant folding. The yolk sac forms the primitive abdomen and, the gastrointestinal tract is derived from the endoderm of the trilaminar embryo and elongates from the buccopharyngeal and cloaecal membrane (Bhatia et al. 2020). This highlights the importance of the yolk sac because it can visibly show sonographically using a transvaginal ultrasound at five weeks (Donovan and Bordoni, 2020). The organs in the digestive system derived from all of the germ layers and the three regions: foregut, midgut and hindgut vary in vascular blood supply. The foregut initiates from the mouth (oral cavity) to the duodenum; first part of the small intestine and receives blood via the celiac artery (Bhatia et al., 2020). The oral cavity formed from the buccopharyngeal membrane. The midgut is formed from the lateral embryonic folding and is from the mid-duodenum to the 75% of the transverse colon in the large intestine and receives blood from the superior mesentery artery (Bhatia et al., 2020). The hindgut forms the remainder of the colon to the upper anus and receives blood from the inferior mesentery artery (Bhatia et al. 2020). The eye pits and limb buds become apparent during the fourth and fifth week. Besides, the gonads can also be visualised but are not recognised until the seventh week, 42nd day. The development of the limbs, gastrointestinal tract further occurs during the sixth week. An insight into the bone (Idham) formation and Lahm (intact flesh and muscles). Bone formation initiates in the seventh week of the embryonic period whereby the cartilaginous skeleton is developed and gives a rise of the facial characteristics and a human-like body (Bett et al. 2013). This is progressed further in the eighth week where features become definitive. The approximate size of the baby is 10mm (Curran, 2019). The eighth week marks the end of the Takhliq (embryonic phase) and the introduction of the foetal period. The cartilage placed with bones via the ossification process where it initiates in the femur and then the sternum and maxilla (Sadaat, 2009). The hands become more visible and the fingers have spatial plane. The head connects the neck with the trunk (Betts et al. 2020; An-Najjar, 2005). The gonads appear more but the gender cannot be determined. The muscles differentiated via myogenesis causes muscle contraction. Allah has stated in Surah Al Muminoon, verse 14 that the muscles need to develop following the bones to form ‘another creature’ which signifies the significant changes that occur where it becomes more human-like (Moore, 1986). Initial movements then take place in the upper and lower extremities of the human body (embryology.cn. 2020b). Concomitantly, this been described by the Prophet (peace be upon him) more than 1400 years ago. It was narrated by Huzaifah (may Allah have mercy upon him) that the Prophet (peace be upon him said): “When 42 nights have passed over the conception, Allah sends an angel to it, who shapes it (into human form) and makes its ears, eyes, skin, muscles and bones. Then he says; ‘O Lord, is it male or female?’, and your Lord decides what He wishes and the angel records it.” [Sahih Muslim] Therefore, all human features are apparent and have primordial for internal and external organs by the end of week eight. The baby reaches 1.6 cm with a fully developed skeleton and flesh muscles and skin (Curran, 2019).  Figure 5: Embryo at 8 weeks during first trimester (Shiel, 2009) An insight into the Al-Nashaa (foetal stage) The Nasha initiates during the ninth week where continuous development of the foetal body occurs. It consists of Al Nasha Khalaqakha that happens between week 9 and 26 and Al Hadana Al Rahamiya - 26 weeks till full birth uterine incubation (Sadaat, 2009). Al Nasha Khalaqaha consists of rapid growth and development after the 12th week and, the approximate size of the foetus is 5.3 cm (Curran, 2019). The body becomes more balanced due to the presence of the limbs, nails, face and head; there is an appearance of lanugo hair (An-Najjar, 2005; Sadaat, 2009). Organs of the gastrointestinal, reproductive and urinary systems are presented and distinguishable due to the cloaca over the weeks (Kruepunga et al. 2018). For instance, the kidneys that filter and produce urine, the external genitalia whereas the placenta become independently functional (Moore, 1986, An-Najjar 2005). The formation of blood cells, haematopoiesis, now occurs in the bone marrow (An-Najjar, 2005). Also, there is an increase in the movement of the voluntary muscles can be felt by the mother. The intestines move from the umbilical cord to the abdominal cavity (Moore, 1986). Figure 6 presents an image of the foetus at 16 weeks and apoptosis occurs in the ectoderm and mesoderm and; this causes the paddled hands to produce fingers and toes.  Figure 6: The foetus during the second trimester at 16 weeks (Weil, 2009) The phase of Al Hadana al rahima is the remainder of the foetal period until labour (Sadaat, 2009). During this period, the baby can survive and; ‘settle’ without a placenta during the last three months and, the uterus provides a hand of support during the intrauterine development and growth of various organs till the ‘specified term’ as Allah (The Most High) states: (Moore, 1986). "O People, if you should be in doubt about the Resurrection, then [consider that] indeed, We created you from dust, then from a sperm-drop, then from a clinging clot, and then from a lump of flesh, formed and unformed - that We may show you. And We settle in the wombs whom We will for a specified term, then We bring you out as a child, and then [We develop you] that you may reach your [time of] maturity. And among you is he who is taken in [early] death, and among you is he who is returned to the most decrepit [old] age so that he knows, after [once having] knowledge, nothing. And you see the earth barren, but when We send down upon it rain, it quivers and swells and grows [something] of every beautiful kind." [Quran, Surah Al-Haj, 22:5] In Surah al Zumr, Allah states: “He created you from one soul. Then He made from it its mate, and He produced for you from the grazing livestock eight mates. He creates you in the wombs of your mothers, creation after creation, within three darknesses. That is Allah, your Lord; to Him belongs dominion. There is no deity except Him, so how are you averted” [Quran, Surah Al Zumr, 39:6] The use of the term three darkness indicates the placenta and the membranes that surround the baby: the anterior abdominal wall, the uterine wall and amnio-chorionic membrane (Sadaat, 2009). During the sixth month, the neurons become fully developed and the body is covered with a fatty adipose tissue layer and the amniotic fluid increases (Moore, 1982). This thickens during the seventh month. The Optic Chiasma also is known as the decussation of the optic nerves connects with the posterior brain (An-Najjar, 2005). The internal structures of the eye, for instance, the conjunctiva, lacrimal glands, choroids, sclera, and cornea are formed and are surrounded externally with the eyelids (An-Najjar, 2005). The pupil are generated from the thinning of the tunica vasculosa of the eyeball (An-Najjar, 2005). In the eighth month, the hair and foetal size increases and the lanugo disappear, the nails and lungs become fully developed (An-Najjar, 2005). The proximal humeral epiphysis ossification centre can be visualized at 38 weeks. At 41 weeks, the foetus is estimated to weigh 8.3 pounds and height 52.7cm from head to toe (Curran, 2019). This highlights the various transformations that take place during the Nasha phase hence it being the longest period during pregnancy.  Figure 7: The foetus at 32 weeks during the third trimester period (Wiel, 2009) Therefore, all of this research indicates that the Quran is a source of guidance and living evidence for humanity. The embryonic and foetal period has vividly described by Allah (The Most High), how a baby transitioned from a nutfah amshaj (fertilization of the egg and sperm) to takhliq (embryonic phase) to the Nashah (foetal phase). The concept of human development has only been unrevealed following the microscopic invention where significant discoveries found have been concomitantly mentioned in the Quran suggesting it is the word of Allah (The Most High). It is fascinating how a single fertilized egg cell can transform into a baby comprising of various complex organ systems that interconnect with one another. "We shall show them Our signs on the horizons and within themselves until it will become clear to them that it is the Truth. Does it not suffice that your Lord is Witness over all things?" [Quran, Surah Fussilat 41:53] Next month, I will share with you the next section of my research in my personal time which consists of an anatomical and physiological understanding on the senses that allow us to hear, see, listen, smell and feel and will connect with evidence from the Quran and Hadith: “Then He proportioned him and breathed into him from His [created] soul and made for you hearing and vision and hearts; little are you grateful.” [Quran, Surah Sajdah, 32:9] References Alberts B, Johnson A, Lewis J, Raff, M., Roberts, K., and Walter, P. (2002) Molecular Biology of the Cell. 4th ed. New York: Garland Science. Ale-Shaikh, S. (2010) Al-Kutub As-Sittah USA: Darrussalam Al-Kirmani, M. (1981) Al-Kawakib Al-Darari fi Sharh Sahih al-Bukhari Beirut: Dar Ihya al-Turath al-Arabi. Al-Maraghi, A. (1946) Tafsir Al-Maraghi Cairo: Maktabah Al-Mustafah Al Bab Al Halabi. Al-Qismi, J., (2003) Tafsir al-Qasimi: Al-Musamma Mahasin Al-Ta'wil. Dar Ihya al-Kutub al-Arabiya Al-Razi, M. (1981) Tafsir al-Kabir wa Mafatih al-Ghaib Beirut: Dar Al-Fikr. Al-Razi, M. (2010) Mukhtar al-Sihah Beirut: Dar Al-Fayha Al-Shami, S. (2015) Mualim Al-Sunnah Al-Nabawiyah Damascus, Dar Al-Qalam. Al-Suyuti, J. and al-Mahalli, J. (2007) Tafsir Al-Jalalayn Jordan: Royal Aal Al Bayt Institute of Islamic Thought Al-Tabari, A. (2001) Tafsir Al Tabari: Jami Al Bayan An Ta'Wil Aayi al Qur'an. USA: Darussalam An-Najjar, Z. (2005) Wonderful Scientific Signs in the Qur’aan UK: Al Hijaz Betts, J., Young, K., Wise, J., Johnson, E., Poe, B., Kruse, D., Korol, O., Johnson, J., Womble, M., DeSaix, P. (2013) Anatomy and Physiology, USA: OpenStax. Bhat, A. (2016) Human Psychology (fitrah) from Islamic Perspective I n t e rn a t io na l J ou rna l o f Nu s an ta ra I s la m 4 (2) p. 6 1 -74. Bhatia, A., Shatanof, RA. And Bordoni, B. (2020) Embryology, Gastrointestinal. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537172/ Capanna, E., (1999) Lazzaro Spallanzani: At the roots of modern biology. Journal of Experimental Zoology, 285(3), pp.178-196. Carlson, B., (2014) Placenta. Reference Module in Biomedical Sciences,. Chaabani, H., (2018) New insights into human early embryo development: a particular theoretical study. International Journal of Modern Anthropology, 2(11), p.14. Curran, M. (2019) Fetal Development Available from http://perinatology.com/Reference/Fetaldevelopment.htm Denker, H., 1976. Formation of the Blastocyst: Determination of Trophoblast and Embryonic Knot. Current Topics in Pathology, pp.59-79. Dockter, J., (1999) 3 Sclerotome Induction and Differentiation. Current Topics in Developmental Biology, pp.77-127. Donovan, M. and Bordoni, B. (2020) Embryology, Yolk Sac. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK555965/ embryology.ch (2020a) ‘7.2 The trilaminar germ disk (3rd week) Available online: http://www.embryology.ch/anglais/hdisqueembry/triderm01.html embryology.ch (2020b) ‘8.4 The most important events in the third to eighth developmental weeks’ Available online: http://www.embryology.ch/anglais/iperiodembry/evenement06.html Faber, J. and Anderson, D., (2010) The placenta in the integrated physiology of fetal volume control. The International Journal of Developmental Biology, 54(2-3), pp.391-396. Ganten, D., Ruckpaul, K., Birchmeier, W., Epplen, J., Genser, K., Gossen, M., Kersten, B., Lehrach, H., Oschkinat, H., Ruiz, P., Schmieder, P., Wanker, E. and Nolte, C. (2005) Dermomyotome. In: Encyclopedic Reference of Genomics and Proteomics in Molecular Medicine. Springer, Berlin, Heidelberg. Gerton, J. L., and Hawley, R. S. (2005) Homologous chromosome interactions in meiosis: Diversity amidst conservation. Nature Reviews Genetics 6, p. 477–487 Gilbert, SF. (2000) Developmental Biology. 6th edition. Sunderland (MA): Sinauer Associates; 2000. Giovanni, P. (2003) Embryogenesis of vertebrates and the theory of the endoderm as secondary layer: Morphologic and molecular evidence, Italian Journal of Zoology, 70:4, p. 281-289. Gittenberger-de Groot, A., Bartelings, M., Deruiter, M. and Poelmann, R., 2005. Basics of Cardiac Development for the Understanding of Congenital Heart Malformations. Pediatric Research, 57(2), pp.169-176. Griffiths, S. and Campbell, J., (2015) Placental structure, function and drug transfer. Continuing Education in Anaesthesia Critical Care & Pain, 15(2), pp.84-89. Hafez, S., (2017) Comparative Placental Anatomy. Progress in Molecular Biology and Translational Science, pp.1-28. Hassold, T. and Hunt, P., (2001) To err (meiotically) is human: the genesis of human aneuploidy. Nature Reviews Genetics, 2(4), pp.280-291. Hoekstra, C., Zhao, Z., Lambalk, C., Willemsen, G., Martin, N., Boomsma, D. and Montgomery, G., (2007) Dizygotic twinning. Human Reproduction Update, 14(1), pp.37-47. Hooke R. (1665) Micrographia: or some physiological descriptions of minute bodies made by magnifying glasses, with observations and inquiries thereupon. Courier Corporation. Hossain, Mohammad. (2018). Structure Of Human Skeleton Exhibits The Mysterious Love Of Allah (SWT) To Prophet Muhammad (SAW). Ar-Raniry International Journal Of Islamic Studies. 5 (1) p.13 - 39 https://www.sciencedirect.com/science/article/abs/pii/S0143400498800465 Hyun, I., Munsie, M., Pera, M., Rivron, N. and Rossant, J., 2020. Toward Guidelines for Research on Human Embryo Models Formed from Stem Cells. Stem Cell Reports, 14(2), pp.169-174. Ibn Asyur, M. (1984) Tafsir al-Tahrir wa al-Tanwir. Tunisia: Dar al-Tunisiyah. Ibn Hajar Al Asqalani, A. (1997) Fath Al-Bari – Sharh Sahih Al-Bukhari USA: Darussalam. Ibn Kathir (2014) ‘Stories of the Prophet’ USA: CreateSpace Ibn Kathir, I. (1980) Tafsir al-Quran al-Azim. Cairo: Maktabat Al-Nahdah Al-Islamiyah. Ibn Manzur, M. (1988) Lisan Al-Arab Al-Muhit Beirut: Dar Al-Yil Ibn Manzur, M. (2000) Lisan Al Arab Beirut Dar Sader Ibn Qayyim Al Jawziyah, M. (1960) Al-Tabyan fi Aqsam Al-Quran Maktab al- Raiyad Al-Hadith Ing, N., Francis, H., Mc Donnell, J., Amann, J. and Michael Roberts, R., (1989) Progesterone Induction of the Uterine Milk Proteins: Major Secretory Proteins of Sheep Endometrlum1. Biology of Reproduction, 41(4), pp.643-654. James, J., (2014). Overview of Human Implantation. Pathobiology of Human Disease, pp.2293-2307. Jarzembowski, J., (2014) Normal Structure and Function of the Placenta. Pathobiology of Human Disease, pp.2308-2321. Jenkins, S., Mukherjee, S. and Heyer, W., (2016) DNA Repair by Homologous Recombination. Encyclopedia of Cell Biology, pp.456-467. Kahane, N., Ribes, V., Kicheva, A., Briscoe, J. and Kalcheim, C., 2013. The transition from differentiation to growth during dermomyotome-derived myogenesis depends on temporally restricted hedgehog signaling. Development, 140(8), pp.1740-1750. Kauppi, L., Jasin, M. and Keeney, S., (2012) The tricky path to recombining X and Y chromosomes in meiosis. Annals of the New York Academy of Sciences, 1267(1), pp.18-23. Keele, K. D., Leonardo, & Pedretti, C. (1978). Leonardo da Vinci, corpus of the anatomical studies in the collection of Her Majesty the Queen at Windsor Castle. London, Johnson Reprint Co. Keynes, G. (1966) The Life of William Harvey. New York: Oxford University Press. Kruepunga, N., Hikspoors, J., Mekonen, H., Mommen, G., Meemon, K., Weerachatyanukul, W., Asuvapongpatana, S., Eleonore Köhler, S. and Lamers, W., 2018. The development of the cloaca in the human embryo. Journal of Anatomy, 233(6), pp.724-739. Kuo, D. and Lai, Y., 2018. On the origin of leeches by evolution of development. Development, Growth & Differentiation, 61(1), pp.43-57. Leese, H., (1994) Early human embryo development. Journal of Biological Education, 28(3), pp.175-180. Lillie, F., (1914) Studies of fertilization. VI. The mechanism of fertilization in arbacia. Journal of Experimental Zoology, 16(4), pp.523-590. Longo, L. and Reynolds, L., 2010. Some historical aspects of understanding placental development, structure and function. The International Journal of Developmental Biology, 54(2-3), pp.237-255. Marikawa, Y. and Alarcón, V., (2009) Establishment of trophectoderm and inner cell mass lineages in the mouse embryo. Molecular Reproduction and Development, 76(11), pp.1019-1032. Marques P, Skorupskaite K, George JT, Anderson, R. (2018) Physiology of GNRH and Gonadotropin Secretion. In: Feingold KR, Anawalt B, Boyce A, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279070/ Marston, A. and Amon, A., (2004) Meiosis: cell-cycle controls shuffle and deal. Nature Reviews Molecular Cell Biology, 5(12), pp.983-997. Moore, K.L. (1982) The Developing Human. ClinicalIy Oriented Embryology, 3rd ed. Philadelphia: W.B. Saunders. Moore, L. (1986) A Scientist's Interpretation Of References To Embryology In The Qur'an. The Journal of IMA 18. Muench, M., Kapidzic, M., Gormley, M., Gutierrez, A., Ponder, K., Fomin, M., Beyer, A., Stolp, H., Qi, Z., Fisher, S. and Bárcena, A., (2017) The human chorion contains definitive hematopoietic stem cells from the fifteenth week of gestation. Development, 144(8), pp.1399-1411. Niakan, K., Han, J., Pedersen, R., Simon, C. and Pera, R., (2012) Human pre-implantation embryo development. Development, 139(5), pp.829-841. Nwabuobi, C., Arlier, S., Schatz, F., Guzeloglu-Kayisli, O., Lockwood, C. and Kayisli, U., (2017) hCG: Biological Functions and Clinical Applications. International Journal of Molecular Sciences, 18(10), p.2037. O'Connor, C. (2008) Meiosis, genetic recombination, and sexual reproduction. Nature Education 1(1):174 Ohkura, H., (2015) Meiosis: An Overview of Key Differences from Mitosis. Cold Spring Harbor Perspectives in Biology, 7(5), p.a015859. Pansky, B. (1982) Review of Medical Embryology. USA: Macmillan. Pleasure, J., Pleasure, D. and Pleasure, S., 2017. Trophic Factor, Nutritional, and Hormonal Regulation of Brain Development. Fetal and Neonatal Physiology, pp.1326-1333.e3.Pocket Dentistry (2017) Growth and Development. Available from: https://pocketdentistry.com/growth-and-development-2/ Rahman, Z. (2012) The Role Of Fitrah As An Element In The Personality Of A Da’i In Achieving The Identity Of A True Da’I. International Journal of Business and Social Science 3 (4) p165-175 Raju, G., Chavan, R., Deenadayal, M., Govindarajan, M., Gunasheela, D., Gutgutia, R., Haripriya, G., Patel, N. and Patki, A., 2013. Luteinizing hormone and follicle stimulating hormone synergy: A review of role in controlled ovarian hyper-stimulation. Journal of Human Reproductive Sciences, 6(4), p.227. Rehman B and Muzio M. (2020) Embryology, Week 2-3. Available from: https://www.ncbi.nlm.nih.gov/books/NBK546679/ Reynolds, F., (1998). Drug transfer across the term placenta. Placenta, 19, pp.239-255. Saadat, S. (2009) Human Embryology and the Holy Quran: An Overview. International Journal of Health Sciences 3 (1) p. 103-109. Saini, D. and Yamanaka, Y., (2018) Cell Polarity-Dependent Regulation of Cell Allocation and the First Lineage Specification in the Preimplantation Mouse Embryo. Cell Fate in Mammalian Development, pp.11-35. Schwarzacher, T., (2003) Meiosis, recombination and chromosomes: a review of gene isolation and fluorescent in situ hybridization data in plants. Journal of Experimental Botany, 54(380), pp.11-23. Setiawan, W., Tajab, M. and Chaer, M., (2019) Ruh, Soul, Heart, Mind, and Body in the Perspective of Islamic Educational Psychology. Proceedings of the Proceedings of 1st Workshop on Environmental Science, Society, and Technology, WESTECH 2018, December 8th, 2018, Medan, Indonesia,. Shafei, R., Syrkasheva, A., Romanov, A., Makarova, N., Dolgushina, N., Semenova, M. (2017) Blastocyst Hatching in Humans Ontogenez 48 (1) p. 8-20. Shakir, Z. (2018) ‘The Human in the Quran’ Available from https://renovatio.zaytuna.edu/article/the-human-in-the-quran Shiel, W. (2009) Pregnancy and Fetal Development Available from: https://www.medicinenet.com/image-collection/first_trimester_4_weeks_picture/picture.htm Sieck, G., (2019) Physiology in Perspective: Anatomy and Physiology—Structure and Function in Biology. Physiology, 34(6), pp.379-380. Spurway, J., Logan, P. and Pak, S., (2012) The development, structure and blood flow within the umbilical cord with particular reference to the venous system. Australasian Journal of Ultrasound in Medicine, 15(3), pp.97-102. Vakalova, T., Pogrebenkov, V., Vereshagin, V., Khabas, T. and Revva, I., (2018) Optimising rational chemical analysis for quantitative determination of the composition of clay in soils. Applied Clay Science, 163, pp.153-163. Varga, I. (2017). Embryology Teaching: An Often-Neglected Part Of The Medical Curriculum. Revista Argentina de Anatomia Clinica. 9. 47-51. Vincenten, N., Kuhl, L., Lam, I., Oke, A., Kerr, A., Hochwagen, A., Fung, J., Keeney, S., Vader, G. and Martson, A. (2015) ‘The kinetochore prevents centromere-proximal crossover recombination during meiosis’ eLife 4 e10850 Wollman, A., Nudd, R., Hedlund, E. and Leake, M., (2015) From Animaculum to single molecules: 300 years of the light microscope. Open Biology, 5(4), p.150019. Zulkifli, N. (2017) Al-Ahkam Istinbat Method in the Fatwa of Yusuf Al-Qaradawi for the reform of Islamic Law. International Journal of Science and Research 6 (4) p 337 – 343. A third of my time during COVID-19 lockdown was reading to be efficient with time in my research interests: oncology particularly; in cancer therapeutic modalities and my religion Islam which the majority of the time today is misinterpreted. Hence, the reason why this review is found in the COVID-19 section on my website. This project aims to share a qualitative review for the public on one of my individual-based researches titled 'The link between Medicine and Science with the Glorious Quran - with a focus on anatomy and physiology'. The Quran is the Book of Allah (God) revealed more than 1400 years ago during the month of mercy, Ramadan, to the Seal of the Prophets, Muhammad (peace be upon him) in 610. A medical corpus is developed based upon the two branches of Islam: Quran and Hadith (Sayings of Prophet Muhammad (peace be upon him). Typically, in this day and age, one would read the Quran with English translation to understand what is meant in the Fus-ha (classical Arabic language) of early Tafseer (exegesis) work. The Quran requires an in-depth understanding of its Tafseer to eliminate misunderstandings. The philosophical interpretation of the Quran integrates ma'na (meaning) and isharah (sign) (Amir and Yusoff, 2017). To this day, the Quran is studied; by many scholars. I, as a Muslim, had to read from the primary scriptures of Tafseer by respected scholars within the field to write this article such as Ibn Kathir, Al-Qurtubi, Al-Tabari, Ibn Al-Ashur, Ibn Manzoor and Ibn Hajar Al-Asqalani. This highlights the importance of seeking authentic sources to discuss matters of religion. Similarly, to understand the human body and be able to treat disease requires one to study the structure (anatomy) and function (physiology) at seven levels: molecular, cellular, enzymatic, tissue, organ, system and the whole organism (Sieck, 2019). In the same way, a machine or car would require all compartments necessary to work and manoeuvre optimally. If any organ(s) malfunctioned; it is said one has a disease and will experience symptoms. Thus, knowledge of the different forms of anatomy (functional, radiological and topographical) and physiology is fundamental for physical examination, interpretation of symptoms; and radiological images to provide the correct treatment (Arráez-Aybar et al., 2010). The combination of the dimensions of health and Islam initiates with an analysis of Tawhid (Divine Unity) and influences evolutionary hypotheses to understand disease (Saniotis, 2012; Nesse et al. 2010; Hood and Jenkins, 2008; Melchert, 2011). Allah (The Most High) says in the Quran: “The creation of the heavens and earth is far greater than the creation of mankind. But most of mankind do not know it.” (Quran, 40:57) Al-Qurtubi explains that Allah has created the heavens and the earth, and is greater than the humankind and is capable of resurrecting them. Ibn Ashur (2000) commented how the Qadeer (Most Capable) created the universe and its constituents such as the stars and planets; then he is aqdar (more capable) of creating the human body and resurrecting humans back to life without hesitance due to the size, power and energy they comprise but still, the humanity rejects or not know of this concept. Without doubt, medical knowledge of Galen, Hippocrates and Dioscorides has had a significant impact in medicine and were introduced to the Islamic Empire during the Medieval and Renaissance era through translation via Hunayn ibn Ishaq where various physicians re-vitalised and innovated these findings to logical, evidence-based and experimental models (Faruqi, 2006; Saniotis, 2012). This period was known as the ‘Golden Age of Islamic Civilisation’. In my previous individual-based research titled ‘Medicine Through Islamic History’ where I emphasis the contributions of many physicians and their impact on patient care.  The motivating force of Muslim physicians at the time was using their spiritual and temporal sense to understand the wisdom and creation of Allah by studying the natural phenomena in the Quranic context that encompasses the ethics and ideals of all aspects in human life (Kettani, 1976; Faruqi, 2006; Saniotis, 2012). Furthermore, assumptions made that the Islamic Empire consisted of Muslims alone. However, Faruqi (2006) informed that it was a multicultural society with a range of religions, languages and traditions due to conquering of countries from Africa to Asia to Persia to Arabia and how scholars of different faiths studied and taught under Islam (Faruqi, 2006). Amongst the physicians who studied Galen’s anatomical concepts and human dissection were Abdul Latid Al-Baghdadi in 1200; who improved the anatomical presentations of the bones in the lower jaw and sacrum (Al Ghamdi et al. 2017; Khalique et al. 2019). Ibn Zuhr was otherwise known, as Avenzoar greatly influenced the understanding of anatomy (Abdel-halim, 2005; Support Group, The Renal Patient and Al-Ghazal, 2017). Another physician, Ibn Al Nafis, described the pulmonary blood circulation, the chambers of the heart and the lungs (Akmal et al. 2010). His findings was published in the book by Ibn Sina (Avicenna) titled ‘Canon of Medicine’. (West, 2008; Meyers, 1964). Ibn Al-Quff and Ibn Abu Usaybia were other 13th century physicians who described the heart physiology and function (Amr and Tbakhi, 2007; Dalfardi and Yarmohammadi, 2016). However, the physiology of the pulmonary circulation was known as the ‘lesser circulation’ at the time and was further explained in 1500 by Michael Servetus and Realdo Colombo (Meyerhof, 1935). However, upon researching the discovery of pulmonary circulation, numerous researches presented William Harvey, the Founder of human physiology in the 17th century and he was the one who corrected the errors of Galen on the blood circulation and discovered the function of valves (Schultz, 2002; McMullen, 1995; Boyle, 2007; Bolli, 2019). With all respects to his contributions, other scholars within the field such as Aird (2011) and Faruqi (2006) have implied how Al-Razi described the role of valves in the veins in the 10th century and criticised Galen's anatomical theories. Al-Razi also discussed anatomical illustrations of ventricles and the brain in his book Kitab Al Mansuri Fi Al-Tibb. All of these discoveries of these physicians and others were established, through the clinical observations in the free hospitals they founded (Turner, 1995). They were transferred to the curriculum at medical schools in Europe during the Middle Ages and Renaissance eras to strengthen the climate of learning, scientific thinking and exploration (Centre for Islamic studies, 2002). Therefore, this suggests how William Harvey was exposed to the understanding pf the cardiovascular physiology of the human body. Furthermore, physicians such as Ibn Sina and Al Khawarizima did not only expand the Ancient Greek findings but also made their contributions of their own in other academic areas such as mathematics, physic and chemistry (Mannan and Kahvic, 2010; Hajar, 2013; Nasser et al. 2009; Faruqi, 2006). Thus, God was central in their lives and; they were the trustees who benefited from the world and used it to understand and share their knowledge. Our body cells rely on the photons (light particles) where our hearts and minds form an electromagnetic field that interacts with one another to increase our perceptions and make sense of the world around us. Critics state that the Quran does not consist of evidence of every organ in the body. On the other hand, it is a source of guidance where 20% (1200 verses) of this Glorious book is composed of miracles in science and medicine (Alhinai, 2015). The Quran is a guide for every matter in which humanity faces, thus, even one verse from the Quran serves a foundation for a topic itself. The Quran is also a source of healing of physical ailments and human diseases: cancer, heart disease (Ibrahim et al., 2016). However, it acts as a complementary approach and works hand in hand with modern treatment that comes from the knowledge given by God and; this is little (Ibrahim et al. 2016). Allah (The Most High) states: "And they ask you, [O Muhammad], about the soul. Say, "The soul is of the affair of my Lord. And mankind have not been given of knowledge except a little." [Quran, 17:85] My review aims to cultivate the two grounds: Quran and medicine in understanding the importance of anatomy and physiology of the human body using scholarly views on the Tafseer of the Quran. An understanding and cultural awareness from a moral and ethical perspective can be increased (Gatrad and Sheikh, 2001; Henley and Schott, 1999). The review is sub-divided over six months: embryology and the development of human, five senses, heart, brain, intestines, bone and movement with closing remarks on the 5th of each month at 8pm in the United Kingdom. References Abdel-Halim, R. (2005). Contributions of Ibn Zuhr (Avenzoar) to the progress of surgery. A study and translations from his book Al-Taisir. Saudi medical journal. 26 (9), pp. 1333-9.
Abdul-Rahman, M.S. (2003) Divine Unity (Tawheed) Open Library: MSA Publication Limited Aird, W.C. (2011) Discovery of the cardiovascular system: from Galen to William Harvey Journal of thrombosis and haemostasis 9 (1). Akmal, M., Zulkifle, M. and Ansari, A. (2010)Ibn Nafis - A Forgotten Genius in the Discovery of Pulmonary Blood Circulation. Heart Views. 11 (1) pp. 26-30. Alghamdi, M., Ziermann, J. and Diogo, R., (2017) An untold story: The important contributions of Muslim scholars for the understanding of human anatomy. The Anatomical Record, 300(6), pp.986-1008. Alhinai, S. (2015). Scientific and Medical Miracles in the Human Body. Available online: https://www.researchgate.net/publication/281277302_Scientific_and_Medical_Miracles_in_the_Human_Body [15th May 2020] Amir, S. and Mohd Yusoff, Z., (2017) The Contemporary Scientific Interpretation of Al-Quran: A Review on Al-Sha’rawi’s Method in Tafsir. International Journal of Quranic Research, 9(1), pp.51-66. Amr, S. and Tbakhi, A., (2007) Ibn Al-Nafis: Discoverer of the Pulmonary Circulation. Annals of Saudi Medicine, 27(5), pp.385-387. Arráez-Aybar, L., Sánchez-Montesinos, I., Mirapeix, R., Mompeo-Corredera, B. and Sañudo-Tejero, J., (2010) Relevance of human anatomy in daily clinical practice. Annals of Anatomy - Anatomischer Anzeiger, 192(6), pp.341-348. Bolli, R., (2019) William Harvey and the Discovery of the Circulation of the Blood. Circulation Research, 124(9), pp.1300-1302. Boyle, M., (2008) Harvey in the sluice: from hydraulic engineering to human physiology. History and Technology, 24(1), pp.1-22. Centre for Islamic studies (2002) ‘Physiology’ Available online: https://islamic-study.org/physiology/ [20th April 2020] Dalfardi, B. and Yarmohammadi, H., (2014) Ibn al-Quff (1233–1286 AD), a medieval Arab surgeon and physician. Journal of Medical Biography, 24(1), pp.36-37. Fadel, H.E. (2008) What is Islamic medicine? How does it relate to contemporary medicine? Journal to Islamic Medication Association 40: 57. Faruqi, Y. (2006) Contributions of Islamic scholars to the scientific enterprise. International Education Journal. 7(4), pp. 391-399. Gatrad, A. and Sheikh, A. (2001) Medical ethics and Islam: principles and practice. Archives of Disease in Childhood, 84(1), pp.72-75. Hajar, R., (2013) The air of history (Part V): Ibn Sina (Avicenna): The great physician and philosopher. Heart Views, 14(4), p.196. Henley, A. and Schott, J. (1999) Culture, religion and patient care in a multi-ethnic society. Age Concern England: London, pp. 1–30. Hood, E. and Jenkins, K., (2008) Evolutionary Medicine: A Powerful Tool for Improving Human Health. Evolution: Education and Outreach, 1(2), pp.114-120. Ibn Ashur (2000) Tafsir al Tahrir wal Tanwir. Ibrahim, M. A., Shah, M. and Mohd, R. A. (2016). Concept Of Shifa In Al-Quran : Quranic Medicine Approach In Healing Physical Ailment. Al-Qanatir International Journal of Islamic Studies, 6 (1). Kettani, M.A. (1976) Moslem contributions to the natural sciences. Impact of Science on Society, 26(3), 135-147. Khalique, A., Siddiqui, M. and Ashraf, M. (2019) Irsal-E-Alaq (Hirudotherapy) in Unani system of medicine and modern medicine an overview. International Journal of Unani and Integrative Medicine, 3(1) pp. 1 – 6. Mannan, A. and Kahvic, M. (2010) Ibn Sina : a tribute. The Gulf Journal of Oncology 7 pp. 60-63. McMullen, E. (1995) Anatomy of a physiological discovery: William Harvey and the circulation of the blood. Journal of Royal Society of Medicine, 88: pp. 491-498. Melchert, C. (2011) 'God Created Adam in His Image' Journal of Qur'anic Studies 13 (1), pp. 113 – 124. Meyerhof, M. (1935) Ibn An-Nafis (XIIIth Cent.) and his theory of lesser circulation. Isis, 23(1), pp. 100-120. Meyers, E. A. (1964) Arabic Thought and the Western World in the Golden Age of Islam. New York: Frederick Ungar Publishing Co. Nasser, M., Tibi, A. and Savage-Smith, E., (2009) Ibn Sina's Canon of Medicine: 11th century rules for assessing the effects of drugs. Journal of the Royal Society of Medicine, 102(2), pp.78-80. Nesse, R., Bergstrom, C., Ellison, P., Flier, J., Gluckman, P., Govindaraju, D., Niethammer, D., Omenn, G., Perlman, R., Schwartz, M., Thomas, M., Stearns, S. and Valle, D., 2009. Making evolutionary biology a basic science for medicine. Proceedings of the National Academy of Sciences, 107(suppl_1), pp.1800-1807. Saniotis, A., (2012) Islamic Medicine and Evolutionary Medicine: A Comparative Analysis. Journal of the Islamic Medical Association of North America, 44(1). Schultz, S., (2002) William Harvey and the Circulation of the Blood: The Birth of a Scientific Revolution and Modern Physiology. Physiology, 17(5), pp.175-180. Shakir, Z. (2018) The Human in the Qur’an. Available online: https://renovatio.zaytuna.edu/article/the-human-in-the-quran [12th May 2020] Sieck, G., (2019) Physiology in Perspective: Anatomy and Physiology—Structure and Function in Biology. Physiology, 34(6), pp.379-380. Support Group, The Renal Patient and Al-Ghazal, S. (2017). Islamic History & Medicine: The Life of Ibn Zuhr (1094-1162) Muslim Physician, Surgeon & Poet. Available online: https://www.researchgate.net/publication/312588286_Islamic_History_Medicine_The_Life_of_Ibn_Zuhr_1094-1162_Muslim_Physician_Surgeon_Poet [15th May 2020] Turner, R. H. (1995) Science in Medieval Islam: An Illustrated Introduction. Austin: University of Texas Press. West, J., (2008) Ibn al-Nafis, the pulmonary circulation, and the Islamic Golden Age. Journal of Applied Physiology, 105(6), pp.1877-1880. |
Archives
February 2021
Categories
All
|
 RSS Feed
RSS Feed